Energy for Health, Vol. 23, 2023
Dr.ssa Sisti Valentina Maria
Abstract
This paper reports the findings of an observational study investigating the efficacy of pulsed electromagnetic fields (PEMF) in treating osteoarthritis (OA). OA is a degenerative joint condition which mainly affects a significant number of older dogs, leading to discomfort and reduced mobility. magnetotherapy has become a more widely accepted complementary intervention in veterinary medicine in the alleviation of pain and enhancement of joint functionality.
In this study, an analysis was conducted on a representative sample of ten dogs afflicted with OA, which were subjected to magnetotherapy treatments, two sessions per weeks, for a duration of six weeks. The principal indicators of interest included the degree of pain on palpation and the degree of lameness, joint mobility, muscle circumference and the dogs’ level of participation and happiness. Validated assessment instruments were employed, and clinically significant data was gathered.
The observational study produced evidence showing a notable reduction in joint pain and an improvement in joint mobility for dogs treated with magnetotherapy. Additionally, pet owners reported an increase in their pets’ participation and happiness levels.
This study provides encouraging evidence for magnetotherapy’s effectiveness as a therapeutic option for treating joint pain in dogs.
Introduction
Osteoarthritis in Dogs
Osteoarthritis (OA) in dogs is an extremely vast and complex pathology belonging to the orthopedic field. It occurs with extreme frequency in daily outpatient practice. Epidemiological studies report an incidence of OA in dogs ranging between 8% and 20%.
The most significant data of recent scientific research now set aside the old theories according to which OA is a form of senescence or joint wear exclusively of elderly subjects.
The new theories on the pathogenesis of these adult/elderly subjects are currently based on the conception that mediators with a destructive value characterize OA, which act in constructive interaction thanks to self-amplifying mechanisms capable of defeating substances with anabolic and reparative activity. In this context, free radicals assume significant importance and seem to be the cause of the degenerative and inflammatory alterations characteristic of arthrosis in dogs of a certain age. We therefore speak of multifactorial etiology characterized by multiple risk factors.
According to the etiopathogenesis, arthropathies are divided into inflammatory: infectious (bacterial, viral, fungal) and non-infectious (immune-mediated erosive and non-erosive); and non-inflammatory, with consequent effects on their primary localization and symptomatology. Inflammatory arthropathies primarily affect the articular components, the synovium, the ligaments and secondarily the cartilage and subchondral bone. In non-inflammatory (non-neoplastic) forms, on the contrary, the tissues involved are cartilage and bone.
Inflammatory arthropathies are also generally polyarticular (shoulder, elbow, hip), but immune-mediated ones have instead a symmetrical bilateral involvement (carpus and tarsus). The symptoms appear variable. There is lameness in relation to the degree of chronicity of the lesion.
If the OA is of inflammatory origin, there is the presence of swollen, warm, and painful joints, with the risk, in the case of bacterial forms, of hesitating in edematous formations inside the limb and osteomyelitis caused by the erosion of the cartilage matrix induced by pathogenic enzymes or released by leukocytes destroyed by bacteria. Instead, deformation of the joints characterizes the OA of immune-mediated origin; the periarticular soft tissues weaken to the point of sometimes causing rupture of ligaments or tendon supports. In any case, among the different clinical forms, pain is the main manifestation related to the types of osteoarthritis.
OA involves all dogs’ races without distinction and affects all age groups. Bacterial or tick-borne forms can easily affect even young subjects.
To arrive at a precise diagnosis, therefore, in addition to an accurate anamnesis, an in-depth clinical examination and the support of instrumental diagnostic investigations such as: radiographic examinations, arthrocentesis, arthroscopy, culture and serological tests are required. Thanks to increasingly in-depth knowledge about the etiopathogenesis of OA and increasingly innovative diagnostic techniques, we are moving towards a combined medical therapy.
These are different interventions but with a synergistic effect to act on three main objectives: (1) to intervene on the causes that have caused the arthritic degeneration; (2) interfere with the pathogenetic mechanisms that represent the biological substrate of the disease; (3) act to counteract the emerging symptomatology at whatever stage it is.
The primary cause is often treated with surgical therapies to correct the biomechanics of the joint and to try to recover its functionality.
For the other two objectives, a multimodal treatment is used instead, consisting of the integration of different therapies such as: nutritional control both in preventive and therapeutic form: aimed at reducing excess weight that could affect the diseased joints; rehabilitation physiotherapy; pharmacological treatment understood as “pain-oriented” symptomatic therapies (eg: NSAIDs) and “disease-oriented” ones (eg: chondroprotectors).
Physiotherapy rehabilitation is now considered an effective complement to surgical and pharmacological treatments for OA in dogs. It is capable of pursuing six important objectives: 1) improve joint function, correcting alterations and re-educating the patient to walk; 2) reduce muscle contractures and stimulate the trophism of the myotenoligamentous apparatus due to periods of reduced motor activity; 3) increase proprioceptive abilities and exploit the plasticity of the nervous system; 4) stimulate the blood and lymphatic system; 5) enhance muscle trophism; 6) decrease pain.
The application methods are numerous and are often linked to the aptitudes of the veterinary surgeon who performs them, to his availability of space, time, and economics. Among the often-used rehabilitation treatments we find active/passive therapeutic exercises and instrumental techniques: magnetotherapy, laser therapy, TECAR therapy, shock waves, ultrasound therapy, neuromuscular electrostimulation.
Magnetotherapy
The use of magnetic fields dates to Egyptian times. We have considerable evidence of its use also from the Roman period and the Middle Ages. Magnetotherapy is defined by Steiss (1997) as “a form of physical therapy which, by exploiting the interaction between a magnetic field and the body, regulates the electrochemical balance of the cell, restoring the correct membrane permeability; thanks to its bio-regenerating action, it stimulates tissue regeneration and accelerates repair phenomena”.
Not all magnetic fields are the same, a clear distinction is made between constant ones and those that vary over time or pulsating; in general, it is the latter that are used for therapeutic purposes. The effect of magnetotherapy on organisms would be realized at the
level of neurovegetative and cellular metabolic regulation.
The pulsed magnetic fields induce micro-currents which, causing ion exchanges in the cell membranes, restore the correct membrane potential (unbalanced in the case of a pathological cell).
From this restored electrochemical balance of the cell, a correct membrane permeability follows.
The bio-stimulating effect ultimately modulates and accelerates tissue regeneration and repair.
Dragone L. (2015) summarizes the effects of magnetotherapy on the body in: increase in cellular permeability; ionization of protoplasmic molecules and increase of the polarization level; increased permeability to calcium; piezoelectric effect on the bone and stimulation of fibrocartilage calcification; inhibition of bone resorption and earlier callus formation; increased action of osteoblasts; cartilage stimulation; analgesic effect.
By intervening on certain parameters such as the intensity of the field, the frequency of the impulses and the duration of exposure of the body to the pulsed magnetic field, different effects can be achieved: analgesic, anti-inflammatory, biostimulant and repairing.
The fields of application of magnetotherapy are many:
- Treatment of fractures, osteoarthritis, arthritis, consolidation delays.
- Inflammatory processes
- Contractures and muscle spasms
- Vascular alterations
- Pain
- Neurological pathologies (Steiss,1997)
Among the various applications of magnetotherapy, the best known and most studied is the one on the bone. Several studies have shown that magnetotherapy is able to accelerate and/or reactivate the phenomena of bone healing, promoting the proliferation of osteoblasts, local neo-vascularization, and mineralization of the fibrocartilaginous callus (Dragone, 2015; Auer et al., 1983; Carlucci et al., 1978).
Some studies in human medicine have instead questioned the pain-relieving power of this technique (McCarthy et al., 2006), minimizing the encouraging results brought to light by recent clinical studies conducted on the subject. Recent scientific works have been able to confirm how low intensity and frequency pulsed magnetic fields can influence the behavior of different cell types: nerve, endothelial, connective tissue, and muscle. Colciago et al. (2019) analyzed in vitro the biological responses to EMF exposure on cells of the peripheral nervous system. In this work, the effects of electromagnetic fields on cultures of rat Schwann cells (SC) (taken from the sciatic nerve) regarding their viability, proliferation, migration capacity and specific myelin markers were studied.
Research has shown that the exposure of these cells to electromagnetic fields does not cause toxic stimuli, morphological changes or influence their migration and myelinating capacity. On the contrary, prolonged, and repeated exposure over time to low intensity and frequency PEMF fields induces increased proliferation in SCs. Therefore, the use of PEMF could represent a useful tool to improve the regenerative capacities of myelin producing SCs affecting peripheral nerves with significant consequences on the fields of application in medicine, both in preventing degeneration and in promoting nerve regeneration. Although the use of pulsed electromagnetic fields in osteoarticular pathologies is very extensive in daily clinical practice, the underlying mechanisms of action remain partly unknown and complex to reconstruct due to the multiple interactions between the different biological tissues. Unfortunately, the bibliography on this subject is scarce. Some publications on works conducted on osteoblasts (De Mattei M et al., 1999), osteoclasts (Chang K et al., 2003) and on cultures in liquid medium of fibroblast-like cells derived from human peripheral blood mononuclear cells date back to the 1980s (Gómez-Ochoa et al., 2010); however, these works are not sufficient to explain the anti-inflammatory effect of magnetic fields on osteoarthritis processes. In the 2017 Biochemistry and Biophysics Report, a comparative study between electromagnetic fields and low-level laser therapy conducted on mitogen-activated protein kinases is cited in which the powerful healing effect that electromagnetic fields emerge, through the stimulation of protein kinase pathways.
At the end of this article, there is even talk of such a high biological stimulation effect on cells due to magnetic fields, that a moderate use is recommended in terms of time and frequency of use. The need arises to further investigate the effects of magnetotherapy in veterinary medicine as this sector unfortunately does not have enough scientific evidence. Considering the above premises, the
present prospective observational study aims to describe and evaluate the effects of low-frequency and intensity pulsed electromagnetic fields (PEMF) in dogs with osteoarthritis.
Materials and Methods
The study was conducted between September 2021 and September 2022, at: the Rehabilitation Physiotherapy department of the Teaching Hospital of the School of Veterinary Medical Sciences of Camerino, the Futuravet facility (second level) of Tolentino and the Veterinary Clinic (associated studio) of Posatora (AN). Before starting data collection, informed consent was obtained from the owner of each subject.
Population
All patients diagnosed with OA were evaluated by clinical and instrumental examination (radiography) regardless of joint involved, age, race, and weight; the patient were in pharmacological wash-out for at least two weeks. The degree of severity of the pathology was defined based on the radiographic examination, using the Kellgren-Lawrence classification scale.
This scale identifies five degrees of severity: not appreciable, doubtful, minimum, moderate, and severe; we start from a perfect joint, then as we continue along the ladder we see a reduction of the joint space, bone sclerosis, important bone deformation, disappearance of the cartilage and formation of osteophytes.
Study Design
Each patient underwent two magnetotherapy sessions a week distributed equidistantly from each other for a total of twelve sessions. The patients did not undergo any further medical treatments during the physiatric treatment cycle. For the application of low intensity and frequency pulsed electromagnetic fields (PEMF), the portable device PMT QS (ASA Srl, Arcugnano) was used, equipped with Flexa applicators (36 x 21 x 2 cm (L x P x H) – 1.2 kg), programmable frequency from 0.5 to 100 Hz and variable magnetic field intensity from 5% to 100% (from ~2.5 to ~40 Gauss).
The handpieces were placed directly in contact with the anatomical site of the arthrotic lesion by taking advantage of the appropriate elastic bands. The treatment was delivered without requiring any predetermined position of the patient. All patients were treated with the following protocol and device settings: the clinical protocol has thus been set up based on the clinical practice of the center and is conceived in such a way as to initially obtain an analgesic, vascular stimulation, and therefore anti-inflammatory effect; and subsequently by an increasingly bio stimulating effect. The subjects were evaluated at the baseline visit (T0) and at the end of the sixth session (T1) and the twelfth session (T2) of treatment.

Figures 1.1
Patient Whiskey – Example of application of PEMF magnetotherapy at low intensity and frequency.
| Frequency (Hz) | Intensity (%) | Time (Min) | |
|---|---|---|---|
|
First 3 Sessions |
|||
|
Phase 1 |
40 |
33 |
25 |
|
Phase 2 |
70 |
33 |
25 |
|
Next 5 Sessions |
|||
|
Phase 1 |
100 |
10 |
25 |
|
Phase 2 |
60 |
100 |
25 |
|
Last 4 Sessions |
95 |
50 |
45 |
Clinical Outcomes
The following parameters were evaluated for each patient: pain on palpation, degree of lameness, level of participation and happiness, circumference of ipsilateral and contralateral muscle masses, range of motion (ROM) of the treated joint.
Pain on Palpation
By palpation and manipulation of the limb, the different consistency of the muscles, the possible presence of contractures, crackles, or points of evident pain (trigger points) that limit the load or the joint ROM of the patient were evaluated. The degree of pain on palpation was measured using a scale of values (Knap et al., 2008) with a score from 0 to 4:
0 = no sign of pain on palpation
1 = mild pain on palpation
2 = moderate pain on palpation
3 = intense pain on palpation
4 = the subject is in so much pain that the limb cannot be palpated
Degree of Lameness
Lameness, a clinical symptom characterized by irregular gait, was assessed by physical examination using a scale of values ranging from 0 to 5 (Knap et al., 2008):
0 = normal gait
1 = slight lameness
2 = evident lameness without subtracting the limb from the load
3 = severe lameness without removal of the limb from weight bearing
4 = severe lameness with intermittent unloading of the limb
5 = severe lameness with continuous removal of the limb from weight bearing
Level of Participation and Happiness
This qualitative parameter was evaluated by objective clinical examination during visits and by feedback received from the owner.
A scale of values ranging from 0 to 5 was used:
0 = impatience
1 = distrust
2 = fair
3 = good
4 = excellent
5 = complete
Range of Motion (ROM)
The degree of joint mobility was evaluated using an arm goniometer, consisting of two arms hinged together. The reference arm remains fixed while the other has been rotated according to the movement of the joint under examination, the pin is applied to the motor center of the joint. Before proceeding with the measurements, to limit possible errors, the subject was expected to be sufficiently relaxed. The subject was placed in standing position or in lateral recumbency. Each measurement was repeated three times and the mean value was taken. For each patient, the joint angles of maximum flexion and maximum extension of the joint subject to OA were measured. In the case of patients with carpal OA, maximal external rotation was evaluated.
Circumfrence of Muscle Masses
The measurement of the circumference of the articular masses always took place in the same landmarks, for the anterior limb the point was located on the middle third of the humerus while for the rear limb on the middle third of the femur. A specific meter called Girthometer was used to measure muscle mass. This instrument consists of a tape equipped with a spring and relative dynamometer which allows the same force to be applied during measurements. To reduce the measurement error also in this case, the measurement was repeated three times and the mean value was taken. Each measurement was compared to that of the contralateral muscle.
Statistical Analysis
A descriptive statistical analysis of all relevant variables was performed. Continuous variables were summarized by number of patients (N), mean, standard deviation, minimum, maximum. Categorical variables were summarized by number (N) and percentage of patients (%). Differences for all clinical outs were calculated for each patient at the sixth and twelfth treatments using the baseline visit as a reference.
The significance level of the statistical tests was set at 0.05. Parametric tests (e.g., Student’s t-test) were used to analyze continuous variables; when the continuous variables are not normally distributed, the corresponding non-parametric tests have also been performed (e.g., Wilcoxon’s signed-sum ranks test).

Figure 2.1
Patient Whiskey – Radiographic image of left elbow, severe osteoarthritis with osteophytosis cranial to the radial head and humeral condyles with deformation of the condylar joint profile. Pro curvature of radium and ulna.
Results
Ten patients of varying breed and size with a mean weight of 24.5 ± 12.1 kg (Min = 11.4 kg and Max = 45.0 kg) and age of 10.0 ± 3.0 years (Min = 4.0 years, Max = 13.5 years) were enrolled. At the baseline visit, the population had a degree of osteoarthritis of severe degree in 70% of cases, of moderate degree in 20% of cases and of minimal degree in the remaining 10%. The anatomical sites affected by osteoarthritis and treated were the hip (3 cases), the elbow (2 cases), the spine (3 cases), the shoulder (1 case) and the carpus (1 case).
The degree of pain on palpation detected was 2.7 ± 1.3 (Min = 0, Max = 4), while the degree of lameness was evaluated equal to 1.9 ± 1.1 (Min = 0, Max = 4).
At the baseline visit, the mean level of participation and happiness found in the subjects was 2.4 ± 2.0 (Min = 0, Max = 5) points.
The measurements of the circumference of the muscle of the ipsilateral limb and its contralateral limb, the degree of flexion, extension and external rotation of the treated limb are shown in Table 1. In the middle of the treatment cycle (T1), after 6 sessions of PEMF magnetotherapy, the pain on palpation was reduced by an average of 1.5 ± 0.8 points, equal to 52.5% ± 25.8% (p < 0.05).
The degree of lameness decreased by 1.1 ± 0.5 points equal to a reduction of 60.0% ± 30.9% (p < 0.05).
The mean level of participation and happiness increased significantly by 1.4 ± 1.7 points from the baseline value (p < 0.05). The muscle circumference of the treated limb was increased on average by 9.2% ± 6.3%, while that of the contralateral limb by 3.8% ± 5.3%.
The degrees of flexion and extension were evaluated separately for: hip, elbow, spine and shoulder (see Table 2); on average compared to baseline, the degree of flexion decreased by 19% ± 14%, while that of extension by 9.1% ± 8.4%. The degree of external rotation was evaluated in only one individual, at T1 it resulted decreased by 15% compared to T0.
At the end of the treatment cycle (T2) compared to baseline, pain on palpation decreased by 2.3 ± 1.2 points equal to a reduction of 83% (p < 0.05); the degree of lameness improved on average by 1.5 ± 0.8 points equal to 79.7% (p < 0.05), while the level of happiness-participation increased by 1.8 ± 1.9 points.
The muscle circumference of the treated limb was increased by 14.6% ± 7.9% while that of the contralateral muscle by 6% ± 7%. As regards the mobility of the hip, elbow, spine and shoulder joints, flexion increased on average by 28% ± 11% while extension decreased by 17.3% ± 10.3%. Carpal mobility as assessed by external rotation measurement increased by 50%.
The results obtained in the middle and at the end of the treatment cycle are shown in Table 2.
| Mean | SD | Min | Max | |
|---|---|---|---|---|
| Muscle Circumference Limb (cm) | ||||
| Ipsilateral | ||||
| Hip | 30.7 | 6.8 | 24 | 40 |
| Elbow | 23.5 | 6.5 | 17 | 30 |
| Column | 33.7 | 6.1 | 26 | 41 |
| Shoulder | 28 | 0 | 28 | 28 |
| Carpus | 18.5 | 0 | 18.5 | 18.5 |
| Controlateral | ||||
| Hip | 33.2 | 7.1 | 26.5 | 43 |
| Elbow | 26 | 7 | 19 | 33 |
| Column | 36.7 | 7 | 29 | 46 |
| Shoulder | 32 | 0 | 32 | 32 |
| Carpus | 20 | 0 | 20 | 20 |
| Range of Motion (in degrees) | ||||
| Flexion | ||||
| Hip | 55.7 | 4.9 | 50 | 62 |
| Elbow | 47.5 | 2.5 | 45 | 50 |
| Shoulder | 58.3 | 6.2 | 50 | 65 |
| Carpus | 20 | 0 | 20 | 20 |
| Extension | ||||
| Hip | 129.3 | 14 | 111 | 145 |
| Elbow | 144 | 4 | 140 | 148 |
| Column | 121.3 | 24.5 | 92 | 152 |
| Shoulder | 145 | 0 | 145 | 145 |
| External Rotation | ||||
| Carpus | ||||
| 13 | 0 | 13 | 13 |
Table 1
Ipsilateral/contralateral Muscle Circumference and Range of Motion of the Treated Joint of the Baseline Visit Population.
| T0 Mean (SD) | T1 Mean (SD) | T2 Mean (SD) | |
|---|---|---|---|
| Pain | 2,7 (1,3) | 1,2 (0,7) | 0,4 (0,5) |
| Lame | 1,9 (1,1) | 0,8 (0,7) | 0,4 (0,5) |
| Happiness-Participation | 2,4 (2,0) | 3,8 (1,1) | 4,2 (0,9) |
| Limb Circumfrence (cm) | |||
| Ipsilateral | |||
| Hip | 30,7 (6,8) | 33 (6,5) | 34,5 (6,6) |
| Elbow | 25,3 (6,5) | 25,3 (7,2) | 26,3 (7,25) |
| Column | 33,7 (6,1) | 37,3 (4,2) | 38,7 (4,5) |
| Shoulder | 28 (0) | 30 (0) | 31 (0) |
| Carpus | 18,5 (0) | 20 (0) | 22,5 (0) |
| Controlateral | |||
| Hip | 33,2 (7,1) | 34 (7,3) | 34,7 (6,8) |
| Elbow | 26 (7) | 26 (7) | 26,3 (7,2) |
| Column | 36,7 (7) | 38,7 (5,3) | 39 (4,2) |
| Shoulder | 32 (0) | 32 (0) | 32 (0) |
| Carpus | 20 (0) | 22 (0) | 22,5 (0) |
| Range of Motion (in degrees) | |||
| Flexion | |||
| Hip | 55,7 | 46,5 (13,8) | 41,8 (10,6) |
| Elbow | 47,5 (2,5) | 39,5 (5,5) | 35 (5) |
| Column | 58,3 (6,2) | 45,3 (11,6) | 39 (9,4) |
| Shoulder | 52 (0) | 48 (0) | 42 (0) |
| Extension | |||
| Hip | 129,3 (14) | 143 (9,2) | 155 (8,2) |
| Elbow | 144 (4) | 149,5 (2,5) | 162 (4) |
| Column | 121,3 (24,5) | 133,7 (15,6) | 142,3 (14,3) |
| Shoulder | 145 (0) | 150 (0) | 158 (0) |
| External Rotation | |||
| Carpus | |||
| 13 (0) | 11 (0) | 6,5 (0) |
Table 2
Mean value and standard deviation of monitored parameters before, during and at the end of the treatment cycle.
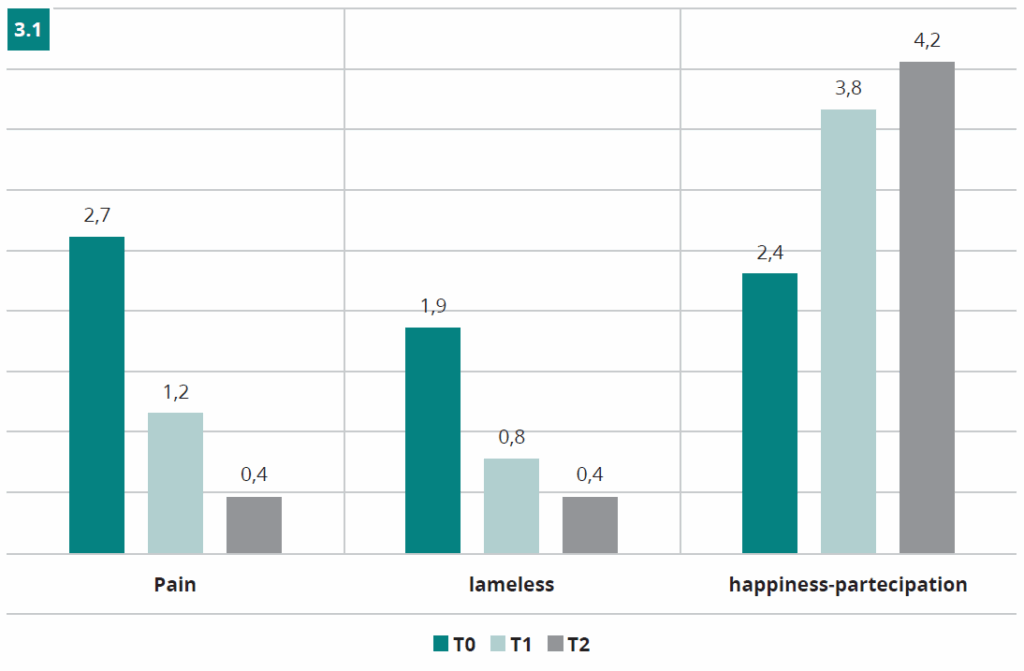
Figure 3.1
Degree of pain, lameness and level of Participation and Happiness found in the population under examination at the Baseline visit (T0) after 6 sessions (T1) and after 12 sessions (T2) of PEMF magnetotherapy.
Discussion
Patients treated with low-intensity and low-frequency PEMF magnetotherapy showed a significant reduction in pain, lameness, participation, and happiness, both in the middle of the treatment cycle and at its end, compared to the data measured at the baseline visit. This was also found in an ever-greater availability, malleability, and willingness of the subjects to undergo PEMF magnetotherapy and this is an indication of clinical positivity.
The increase in joint mobility found during this study is a comforting fact. Regardless of the result achieved at the end of the twelve sessions, it expresses a positive response from the patient to the treatments and suggests the possibility of being able to further improve joint mobility if the subject undergoes a longer and/or maintenance cycle of magnetotherapy.
Although evaluated in only one subject, even the slightest correction of the rotated carpus in valgus suggests a positive interference of the PEMFs with the osteo-articular structures.
It should be remembered that the clinical improvement observed may in part have been influenced by the following factors:
1 – Managing the Patient at Home
After taking a treatment, the owners should manage the patient according to certain rules such as: warm and dry environment; controlled motor activity (avoid jumping, jerking and sudden movements); contained diet for the achievement of normal weight. Underestimating one of these aspects could not allow the achievement of the desired result, in fact it could be the reason for an, albeit minimal, exacerbation of the initial condition, as has been found in some enrolled patients.
2 – The Protocol Used
The one chosen for this work was defined based on previously obtained results and is the one that is applied in the clinical practice of the center. It has been standardized for all patients to avoid a bias if it is customized for each patient. However, it is believed that an adjustment, at each session, of the therapy to the physiological and clinical condition of the patient can lead to obtaining the best results.
This study has demonstrated how it is possible with non-conventional conservative therapy alone to control the clinically appreciable symptoms caused by arthritic processes such as: pain, lameness, degree of happiness-participation, joint mobility, muscle rebalancing. PEMF therapy, used in a controlled and constant manner, can be indicated, both for acute treatment and for long-term maintenance, to counteract arthritic phenomena, allowing patients, especially geriatric subjects, to achieve a better state of well-being, balance, and tranquility.
Although the small number of patients studied, from the results obtained PEMF magnetotherapy has brought improvements regardless of the degree of severity found or the anatomical district affected.
Further investigations, in larger populations, are needed to further validate the obtained results. Furthermore, it would be interesting to study the benefits of the integrated application of PEMF with other physiatric methods such as: laser therapy, neuro-muscular electrostimulation, passive manual techniques, and active exercises in a more or less controlled manner carried out in succession. This therapeutic approach could provide an additional stimulus for all the anatomical districts involved and a strengthening of the mechanism of action of the PEMF therapy itself.
Conclusions
In this observational study, PEMFs proved to be a valuable therapeutic tool in the treatment of OA in dogs. The treated patients, regardless of the degree of severity, age or anatomical site treated, reported an improvement in pain symptoms, an improvement in mobility and quality of life.
Bibliography
- Amaldi U. (2010). Termodinamica onde elettromagnetismo. Zanichelli, 23-26.
- Auer, J. A., Burch, G. E., & Hall, P. (1983). Review of pulsing electromagnetic field therapy and its possible application to horses. Equine veterinary journal, 15(4), 354–360.
- Bockstahler, B., Levine, D., Millis, D. L., & Wandrey, S. O. N. (2004). Essential facts of physiotherapy in dogs and cats. BE Vet Verlag.
- Chang K, Chang WH, Wu ML, Shih C (2003) Effects of different intensities of extremely low frequency pulsed electromagnetic fields on formation of osteoclast-like cells. Bioelectromagnetics 24(6):431–439.
- Colciago A. et al. (2019). In vitro biological responses to electromagnetic fields exposure of peripheral nervous system cells. Energy for Health, 19.
- De Mattei M, Caruso A, Traina GC, Pezzetti F, Baroni T, Sollazzo V (1999) Correlation between pulsed electromagnetic fields exposure time and cell proliferation increase in human osteosarcoma cell lines and human normal osteoblast cells in vitro. Bioelectromagnetics 20(3):177–182.
- Dragone, L. (2015). Fisioterapia riabilitativa del cane e del gatto. Elsevier srl.
- El-Makakey, A. M. et al. (2017). Comparative study of the efficacy of pulsed electromagnetic field and low-level laser therapy on mitogen-activated protein kinases. Biochemistry and biophysics report, 9, 316–321.
- Fox, S. M. (2016). Multimodal management of canine osteoarthritis. CRC Press.
- Gómez-Ochoa, I., Gómez-Ochoa, P., Gómez-Casal, F., Cativiela, E., & Larrad-Mur, L. (2011). Pulsed electromagnetic fields decrease proinflammatory cytokine secretion (IL-1β and TNF-α) on human fibroblast-like cell culture. Rheumatology international, 31(10), 1283–1289.
- Knap et al. (2008). Small Animal Surgery (terza edizione). capitolo 12:22-23.
- Malegori, S. (2001). Fisioterapia riabilitativa nell’artrosi. Inn Vet Med, 1(4), 35-37.
- McCarthy, C. J., Callaghan, M. J., & Oldham, J. A. (2006). Pulsed electromagnetic energy treatment offers no clinical benefit in reducing the pain of knee osteoarthritis: a systematic review. BMC musculoskeletal disorders, 7, 51.
- Millis, D., & Levine, D. (2013). Canine rehabilitation and physical therapy. Elsevier Health Sciences.
- Miolo, A. L. D. A., & Mortellaro, C. M. (2003). Artrosi del cane e stress ossidativo-infiammatorio: dalla clinica al meccanismo. Veterinaria, 17(1), 17-33.
- Mortellaro, C. M., & Miolo, A. L. D. A. (2004). Approccio medico combinato all’artrosi del cane. Veterinaria, 18(3), 9-19.
- Steiss J.E. (1997). Magnetoterapia: Teoria E Principi Di Applicazione. Cinologia 8 (3):19-20.
- Venturini, A. (2008). Le artropatie nel cane: linee guida. Bollettino Aivpa, 2008(2), 7-15.


