Energy for Health, Vol. 25, 2025
Luca Barni, PT, PhD
Department of Physical Therapy and Rehabilitation, University of Florence, Florence, Italy;
PhD in Human Health Sciences, University of Malaga, Spain;
Private Practice, Montecatini Terme, Italy.
Abstract
Background: Tendinous and bursal disorders are frequent sources of musculoskeletal pain and functional impairment. High-power laser therapy (HPLT) is used in rehabilitation settings for its analgesic, anti- inflammatory and biostimulatory effects, which may contribute to tissue repair.
Objective: To evaluate changes in pain, function and ultrasound-documented tissue morphology following laser therapy in patients with tendinous or bursal lesions.
Methods: Five outpatients with ultrasound- confirmed musculoskeletal soft-tissue pathology (mid-portion Achilles tendinopathy, supraspinatus tendinopathy with or without subacromial bursitis, lateral epicondylalgia with partial lesion of the common extensor tendon, and lateral collateral ligament sprain) underwent ten sessions of MLS® M-Hi laser therapy. Pain intensity (VAS), condition-specific functional scores and ultrasound characteristics were assessed before and after treatment.
Results: Mean pain intensity decreased by 67% (VAS −4 points), and functional scores improved in all cases. Follow-up ultrasound showed reduced tendon or ligament thickness when previously increased, more regular fibrillar alignment, reduction or disappearance of hypoechoic areas, and reduction or resolution of bursal effusion and pathological vascularity. No adverse events were reported.
Conclusions: In this observational case series, MLS® M-Hi laser therapy, used as part of a rehabilitation program, was followed by reductions in pain, improvements in patient- reported function and ultrasound changes compatible with tissue repair in tendinous and bursal lesions. Larger controlled studies are required to confirm these findings and to define optimal treatment parameters.
Introduction
Tendinopathies, enthesopathies and bursal disorders are common causes of pain and functional limitation in musculoskeletal practice. These conditions are often characterized by impaired healing, low-grade inflammation and progressive structural disorganization that may delay recovery [1].
Current management typically combines therapeutic exercise, manual therapy, pharmacological interventions and physical modalities within a multimodal rehabilitation approach [2]. Among these, laser therapy is widely used to modulate pain and inflammation, support tissue repair and facilitate functional restoration, particularly when integrated with targeted exercise programs [3].
Despite its extensive clinical adoption, evidence specifically documenting the structural effects of laser therapy on tendons, ligaments and bursae is still limited. Ultrasound imaging, with its ability to assess tendon thickness, fibrillar alignment, vascularity and peritendinous changes, is an essential tool to relate symptom variation to measurable tissue remodeling [4].
Clinical reports that integrate pain and functional outcomes with ultrasound-monitored structural changes may help clarify the potential contribution of photobiomodulation to tendon, ligament and bursal healing in daily rehabilitation practice.
This case series presents five patients with tendinous or bursal disorders treated with laser therapy, focusing on changes in pain, function and ultrasound appearance. Particular attention is given to the description of MLS® M-Hi treatment parameters, in order to facilitate replication of the protocols.
Materials and Methods
All subjects completed a therapeutic cycle of ten sessions over five weeks, performed with the M-Hi laser device (ASA S.r.l., Arcugnano, Italy), a Class IV high-power system of the MLS® (Multiwave Locked System) family. The device emits synchronized 808 nm (continuous or frequency-modulated) and 905 nm (super-pulsed) wavelengths, with a maximum peak power of 270 W and up to 3.3 W average output, and offers different emission modalities that can be adapted to tissue characteristics.
Treatments were administered using manual scanning or fixed-point techniques, selected according to lesion type and anatomical region. All applications employed a 2-cm diameter handpiece (≈3 cm² spot area). Suggested clinical protocols available in the device software were customized for each patient, and one or more parameter sets could be applied within the same session.
When clinically indicated, laser therapy was combined with a homebased exercise program tailored to the underlying condition.
No additional pharmacological therapies were introduced during the treatment period.
Pain intensity was recorded using a 0–10 VAS before and after each session. Functional outcomes were measured with validated, condition- specific questionnaires (VISA- A, QuickDASH, PRTEE, KOOS). A musculoskeletal ultrasound examination was performed before the first session and after completing the treatment cycle by the same experienced radiologist, using standardized protocols. Ultrasound assessment focused on tendon or ligament thickness, echogenicity, fibrillar alignment, vascularity, and bursal or periosteal alterations.
All participants provided informed consent for the use of anonymized clinical and imaging data for research and publication purposes.Case Presentation
Case 1 – Chronic Mid-Portion Achilles Tendinopathy (M, 71)
Clinical Baseline: A 71-year-old male recreational runner presented with chronic pain and swelling of the right Achilles tendon, persisting for several months despite rest, topical treatments and a short course of anti-inflammatory drugs prescribed by his physician. Baseline ultrasound showed fusiform thickening of the mid-portion of the tendon (7.8 mm, versus 6.0 mm on the contralateral side), loss of the normal fibrillar pattern, hypoechoic intrasubstance areas and mild peritendinous effusion, consistent with Achilles tendinopathy. The paratenon was thickened but continuous, and no partial tear was observed.
Treatment: Laser therapy was delivered twice per week for five weeks, with approximately 48 hours between sessions. The treatment targeted the mid-portion and insertion of the Achilles tendon with fixed-point applications (10 points), combined with scanning along the course of the tendon (80 cm2) and over the calf region (100 cm2) corresponding to the main areas of referred pain during work and sports activities. Each session lasted approximately 5–11 minutes (mean ≈ 9 minutes) and delivered a total energy of about 660–1270 J (mean ≈ 1040 J). Considering all scanning and pointby- point applications within each session, the mean session dose was approximately 4.6 J/cm² (range 4.0–5.1 J/cm²). The Achilles tendon region was treated using predefined “Tendinopathy” protocols at 700 Hz or with CPW emission, with intensity between 80% and 100% of maximal output in both scanning and fixedpoint modalities. From the fifth session onward, an additional “Myalgia/ contracture” scanning program at 1500 Hz and 80% power was applied over the calf.
Laser therapy was integrated with a non-supervised home-based exercise program designed for mid-portion Achilles tendinopathy. The program included concentric and eccentric heel-rise exercises with both legs and then with one leg, progressing to single-leg eccentric heel rises using both legs to return to the starting position. Exercises were performed daily, following a progressive loading schedule of 3 × 10 repetitions for the first two weeks and 3 × 15 repetitions for the last three weeks. Continuation of the exercises was recommended if pain remained ≤ 5/10, discomfort subsided after completion, did not persist the following morning and did not progressively increase over subsequent weeks.
Outcomes: Clinical. Pain intensity on the VAS decreased from 7/10 at baseline to 2/10 at the end of the treatment cycle.
Functional. The VISA-A (Victorian Institute of Sport Assessment–Achilles) score increased from 25.5 to 51 (0–100 scale, higher scores indicating better tendon-related function). Ultrasound. Follow-up ultrasound showed a reduction of tendon thickness to 7.0 mm, reappearance of a more regular parallel fibrillar echotexture and disappearance of peritendinous effusion.Case 2 – Left Supraspinatus Tendinopathy with Subacromial Bursitis (M, 44)
Clinical baseline: A 44-year-old male amateur rugby player reported chronic left-shoulder pain and restricted range of motion.
Baseline ultrasound revealed three main findings: multiple punctate hyperechoic microlesions arranged in series at the enthesis of the anterior bundle of the supraspinatus tendon (up to 0.5 mm in size), periosteal irregularities involving the humeral trochiter and extensive subacromial– deltoid bursitis with hyperechoic internal strands causing coracohumeral impingement during abduction, without hypervascularization of the bursal walls.
Treatment: Given the extent of subacromial bursitis, treatment included fixed-point applications along the deltoid to address the bursa, involving the tissue planes between the anterior deltoid and the long head of the biceps tendon (LHBT). Additional scanning was performed along the bursal region and the supraspinatus tendon, moving from caudal to cranial with gentle manual pressure to facilitate fluid drainage towards the axillary lymph nodes. Ten sessions were completed over approximately five weeks. Each session lasted about 6–12 minutes (mean ≈ 10 minutes) and delivered a total energy between 500 and 950 J (mean ≈ 735 J). Considering all scanning and pointby- point applications, the mean session dose was approximately 4.7 J/cm² (range 4.5–4.9 J/cm²). Fixedpoint and scanning applications over the deltoid, subacromial bursa and supraspinatus tendon were delivered using predefined “Bursitis” and “Tendinopathy” protocols with FPW emission, generally at 700 Hz for the tendon and 900 Hz for the bursa, with power at 40% for fixed points and 70–80% for scanning. Laser therapy was combined with a rehabilitation program focused on scapular stabilizers (serratus anterior, middle and lower trapezius) and rotator cuff strengthening, in line with the University Hospitals recommendations for rotator cuff rehabilitation.
Outcomes: Clinical. Pain intensity on the VAS decreased from 6/10 to 2/10 at the end of treatment.
Functional. The QuickDASH score decreased from 23 to 14. The work and performing-arts/sports modules improved from 25 to 0 and from 50 to 6, respectively, indicating less interference of pain with daily and sports activities.
Ultrasound. Follow-up ultrasound demonstrated resolution of the supraspinatus microlesions and remodeling of the humeral trochiter periosteal irregularities. The subacromial– deltoid bursitis was still present but reduced in size (23 × 6.4 mm versus 30 × 8.5 mm at baseline). Clinically, the patient recovered full active abduction and external rotation without pain and progressively returned to sports.
Case 3 – Supraspinatus Tendinopathy with Subacromial Osteophyte and LHB Tendosynovitis (F, 69)
Clinical Baseline: A 69-year-old female presented with chronic left-shoulder pain and nocturnal discomfort limiting daily activities.
Baseline ultrasound showed a small partial-thickness tear of the anterior bundle of the supraspinatus tendon (deep layers IV and V), approximately 2 × 1.5 mm, with minimal subacromial– deltoid bursitis. A marked transudate within the sheath of the LHB was visible, with the tendon continuous along its course. No cortical irregularities or acute lesions were detected.
Treatment: Laser therapy was delivered using a combined scanning and fixed-point modality targeting both the supraspinatus and the long head of the biceps regions. The patient completed ten sessions over approximately seven weeks, with variable intervals resulting in an average frequency of about two sessions per week. Treatment focused on fixed-point applications over the LHB tendon sheath (14 points) and in the area of supraspinatus microcalcifications (14 points), combined with scanning along the course of the supraspinatus tendon (50 cm2) and over the deltoid region (50 cm2) corresponding to referred pain. Each session lasted approximately 7–14 minutes (mean ≈ 11 minutes) and delivered a total energy between about 670 and 1320 J (mean ≈ 1060 J). Across all scanning and point-by-point applications, the mean session dose was approximately 4.0 J/cm² (range 2.9–4.5 J/cm²). All applications used a predefined “Myalgia/contracture” program with FPW emission at 1500 Hz and intensity between 60% and 90%, adjusted according to tolerance and clinical response.
Outcomes: Clinical. Pain intensity decreased from VAS 7/10 at baseline to 3/10 after the treatment cycle.
Functional. The QuickDASH score improved from 86 to 2.3, with restoration of shoulder mobility and daily functional performance.
Ultrasound. Follow-up ultrasound showed no residual supraspinatus tendon lesion, a reduction in LHB tendon sheath effusion and a more homogeneous fibrillar pattern. The patient regained full range of motion and reported the ability to sleep on the affected side without discomfort.Case 4 – Lateral Epicondylitis with Partial Lesion of the Common Extensor Tendon (M, 43)
Clinical baseline: A 43-year-old male factory worker, performing repetitive upper-limb tasks with moderate loads, presented with persistent lateral elbow pain exacerbated by resisted wrist extension.
Baseline ultrasound revealed an anechoic area of approximately 2 × 3 mm, compatible with a partial-thickness lesion of the common extensor tendon at the enthesis, associated with a 6 × 3 mm hypoechoic region bordered by a rim of hypervascularization on power Doppler, consistent with chronic tendinosis.
Treatment: The patient completed ten sessions over approximately four weeks, with intervals of about 2–3 days between applications. Laser applications focused on the tendinous component of the common extensor origin and on selected myofascial trigger points in the extensor compartment of the forearm. In the initial sessions, treatment mainly consisted of scanning applications combined with trigger-point irradiation over the most symptomatic myofascial areas, according to the referred pain pattern. Each session lasted approximately 4–10 minutes (mean ≈ 6 minutes) and delivered a total energy between about 430 and 1030 J (mean ≈ 590 J). Considering all scanning, fixed-point and trigger-point applications, the mean session dose was approximately 3.7 J/cm² (range 3.0–4.5 J/cm²). All laser applications used a predefined “Myalgia/contracture” program with FPW emission, at 1500 Hz, and intensity mainly between 60% and 80% of maximal output for scanning and fixed-point applications. Early trigger-point applications were delivered at 10 Hz and 15% intensity. Parameters were adjusted according to pain provocation and tissue irritability.
Laser therapy was combined with a progressive strengthening program for the forearm extensor muscles, including concentric and eccentric exercises with gradual load exposure and isometric holds of about 5 seconds per repetition. The patient presented with a marked neuropathic pain component; therefore, in addition to laser therapy, neuromodulation with low-frequency electrical stimulation (2 Hz, high-intensity microcurrent in the microampere range, 250 μs pulse duration) was applied along the course of the radial nerve, targeting both its sensorimotor component and the purely motor component via stimulation of the posterior interosseous nerve identified under ultrasound guidance. The combination of neuromodulation and laser therapy yielded the best clinical effect in this patient.
Outcomes: Clinical. At follow-up, pain intensity decreased from VAS 6/10 to 1/10.
Functional. The PRTEE score improved from 57 to 1.
Ultrasound. Follow-up ultrasound showed restoration of the fibrillar tendon architecture at the enthesis, disappearance of the previously observed anechoic defect and absence of vascular signal at the enthesis.
Case 5 – Lateral Collateral Ligament Injury (Right Knee) (F, 64)
Clinical baseline: A 64-year-old female sustained a grade I sprain of the lateral collateral ligament (LCL) of the right knee following a twisting injury.
Baseline ultrasound revealed a partial tear of the external collateral ligament, approximately 3.8 × 2 mm, located above the meniscal region. Mild peri-ligamentous edema was present, without joint effusion or other ligamentous abnormalities.
Treatment: The patient completed ten laser therapy sessions over approximately six weeks. Sessions were generally scheduled twice per week, with rest intervals ranging from 2 to 6 days. In the initial sessions, the patient reported pain irradiating along the iliotibial band and tensor fasciae latae region; treatment therefore focused on scanning applications combined with trigger-point irradiation in these areas. After this irradiated pain pattern resolved (after the first four sessions), therapy was shifted to fixed-point applications and scanning along the entire course of the lateral collateral ligament. Each session lasted approximately 9–20 minutes (mean ≈ 16 minutes) and delivered a total energy between about 600 and 1025 J (mean ≈ 920 J). Considering all scanning, fixed-point and trigger-point applications within each session, the mean session dose was approximately 3.5 J/cm² (range 3.0–4.3 J/cm²), corresponding to an overall mean therapeutic dose per individual application of about 3.43 J/cm². All laser applications were delivered using a predefined “Distortion/contusion” program with FPW emission at 700 Hz, with intensity typically between 50% and 70% of maximal output for scanning (100 c ) and fixed-point applications (14 points). Early trigger-point applications were delivered at 10 Hz and 15% intensity, with parameters adjusted according to pain provocation and tissue response.
Outcomes: Clinical. Pain intensity decreased from VAS 5/10 at baseline to 2/10 after the treatment cycle.
Functional. KOOS subscales improved across all domains for symptoms, pain and function.
Ultrasound. Post-treatment ultrasound showed continuity of LCL fibers in the area of the previous lesion, resolution of peri-ligamentous edema and absence of hypervascularization. The patient returned to daily activities and light recreational exercise without symptom recurrence.
Summary of Results
All five patients completed the treatment cycle without adverse events or laser-related complications. Pain intensity decreased consistently across cases. Baseline VAS scores (at rest or during activity, depending on the case) ranged from 5 to 7 and decreased to 1–3. The mean VAS decreased from 6.0 ± 0.6 to 2.0 ± 0.6, corresponding to a mean reduction of 4 points (≈ 67 ± 9%).
Functional scores improved in all patients. Condition-specific questionnaires (VISA-A, QuickDASH with sport module, PRTEE, KOOS) showed better values at follow-up, with percentage changes relative to baseline ranging from approximately 39% to almost 100%, depending on the initial impairment and the instrument used.
Ultrasound examinations after the treatment cycle documented structural changes in each case, including reductions in increased tendon or ligament thickness, restoration of fibrillar alignment, decreased hypoechogenicity, reduction or resolution of bursitis and reduction or normalization of vascular signals. In three patients, tendon or ligament echotexture approached normal appearance in the region of the previous lesion. In one case, a small residual subacromial–deltoid bursitis was still present despite healing of the primary tendon lesion, without associated clinical worsening.
Individual clinical, functional and ultrasound outcomes are summarized in Table 1.
Discussion
The findings of this Case Series show improvements in pain, function and ultrasound-monitored tissue structure in patients with different musculoskeletal soft-tissue disorders treated with MLS® laser therapy using the M-Hi device. The mean 67% reduction in VAS scores, combined with better functional questionnaire results (VISA-A, QuickDASH, PRTEE, KOOS), indicates a consistent change in symptoms and disability over the treatment period. These clinical changes were accompanied by ultrasound evidence of tissue modification, suggesting that the intervention may have contributed to both symptom modulation and structural evolution, within the limits of an uncontrolled design.Analgesic and Anti-inflammatory Effects
Photobiomodulation therapy (PBMT) has well-described analgesic and anti- inflammatory actions supported by preclinical and clinical literature. Dual-wavelength protocols combining near-infrared continuous and super- pulsed emission, such as those used in MLS® systems, have been reported to modulate nociceptive pathways, reduce COX-2 expression, decrease prostaglandin synthesis and attenuate neurogenic inflammation [3,5]. Studies have also documented increased microcirculation and improved lymphatic drainage, which may promote edema resorption and metabolic clearance in injured tissues [6].
In the present series, the delivered dose per application (generally between 3 and 5 J/cm², depending on tissue depth and lesion location) falls within ranges associated with analgesic and anti-inflammatory effects in tendinopathies and ligament injuries [7,8]. The progressive pain reduction observed across the treatment cycles is compatible with the temporal dynamics of PBMT-mediated modulation of peripheral sensitization, although causality cannot be demonstrated in this design.Structural and Reparative Outcomes
A notable element of this series is the consistent documentation of structural changes on ultrasound, including normalization of fibrillar alignment, reductions in tendon or ligament thickness when previously increased, resolution of hypoechoic areas, disappearance or reduction of pathological vascular signals and absence of ultrasound-detectable defects in regions of previous partial lesions. These observations are in line with clinical reports suggesting that PBMT can influence tendon morphology and extracellular matrix remodeling.
In Achilles and patellar tendinopathy, studies have described reduced tendon thickness, improved fibrillar organization and smaller hypoechoic regions after PBMT, as assessed by diagnostic ultrasound [8; 9]. Similar structural changes have been reported in lateral epicondylalgia and supraspinatus tendinopathy when PBMT is combined with exercise [10]. Experimental work on MLS® and similar protocols provides mechanistic support for these findings. PBMT has been shown to stimulate fibroblast proliferation, promote collagen I synthesis, regulate metalloproteinases and enhance fibroblast migration [11]. In muscle and nerve models, MLS® irradiation modulates oxidative stress, increases ATP production and promotes cytoskeletal reorganization [12-14]. Taken together, these effects are compatible with the structural changes observed in this small series.
Integration with Exercise Therapy
Laser therapy was combined with condition-specific exercise programs in several cases, such as eccentric loading for Achilles tendinopathy, scapular and rotator cuff strengthening for shoulder disorders, and extensor muscle rehabilitation for lateral epicondylitis. The rationale for this integration is that mechanical loading promotes tendon remodeling, while PBMT may improve tolerance to load, reduce pain during rehabilitation and support matrix reorganization [2, 6].
In some cases where exercise could not be immediately intensified due to pain or neuropathic components, PBMT was used initially with or without neuromodulation and allowed subsequent progression of active rehabilitation. This suggests a potential role for high-power MLS® laser therapy as a component of multimodal care, including phases when loading strategies must be temporized.Clinical Implications
The reproducibility of improvements across different anatomical regions in this series suggests that high-power MLS® laser protocols can be applied to a range of tendinous and ligamentous lesions within musculoskeletal rehabilitation. Ultrasound confirmation of tissue changes adds objective information beyond symptom reports and may help clinicians monitor the evolution of lesions and adjust treatment parameters.
The ability to record treatment parameters session by session, as available in the M-Hi system, facilitated precise reporting of the protocols used in these cases and may be useful in future studies aimed at protocol standardization and quality assurance.Limitations and Future Directions
The main limitations of this study are the small sample size, the absence of a control group and the heterogeneity of anatomical regions and associated rehabilitation programs. These factors limit the generalizability of the results and prevent any firm conclusions on efficacy or on the specific contribution of laser therapy compared with exercise, neuromodulation or spontaneous recovery. Ultrasound assessments were performed by a single experienced operator, which supports internal consistency but does not allow evaluation of inter- observer variability.
Future research should include randomized controlled trials with adequate sample size, the use of quantitative ultrasound metrics such as elastography and power Doppler quantification, comparative studies evaluating PBMT alone versus PBMT combined with exercise, and standardized dosing studies for specific tissue types and stages of injury.
Despite these limitations, the convergence of subjective, functional and imaging findings in this series indicates that MLS® M-Hi therapy, used within a structured rehabilitation program, may influence both symptoms and the ultrasound appearance of tendinous and ligamentous lesions.
Conclusion
This case series describes the clinical course of five patients with tendinous or bursal disorders treated with MLS® M-Hi laser therapy integrated into individualized rehabilitation programs. Across cases, pain intensity decreased, functional scores improved and ultrasound findings evolved towards patterns compatible with tissue repair, including normalization of fibrillar architecture, reductions in pathological thickness, resolution of effusion and disappearance of partial-thickness lesions.
These observations suggest that high-power MLS® laser therapy may represent a useful adjunct in musculoskeletal rehabilitation for selected tendinous and ligamentous conditions. Controlled studies are needed to confirm these preliminary findings, to better define dose– response relationships and to refine treatment parameters for different tissues and stages of injury.Acknowledgements
The author wishes to thank all participating patients for their cooperation and adherence throughout the treatment period. Appreciation is extended to the clinical and technical staff for their support in patient management and to the ultrasound specialists for performing standardized imaging assessments. The author also gratefully acknowledges Davide Travalin, Clinical Manager and Bioengineer at ASA S.r.l., for his technical guidance and scientific support during the study.
| Case | Anatomical Area / Diagnosis | VAS (Pre - Post Per Session | VAS (Start - End of Cycle | ΔVAS Cycle (%) | Functional Outcomes (Questionnaire) | Ultrasound Findings (Post-Treatment) |
|---|---|---|---|---|---|---|
|
1 (M, 71) |
Right Achilles tendon – Chronic
enthesopathy with osteophyte |
5.3 → 2.6 |
6 → 2 |
−4 (−67 %) |
VISA-A: 61.5 → 29 (+53 %) |
Reduced tendon thickness (7.8 → 7 mm); osteophyte 4.5 → 3 mm; homogeneous fibrillar pattern |
|
2 (M, 44) |
Left shoulder – Partial supraspinatus lesion (PASTA) + subacromial bursitis |
4.5 → 2.1 |
6 → 2 |
−4 (−67 %) |
Quick-DASH: 23 → 14 (+39 %); Sport module: 50 → 6 |
Resolution of supraspinatus micro-lesions; restored
periosteal contour; bursitis reduced (30×8.5 → 23×6.4 mm) |
|
3 (F, 69) |
Left shoulder – Deep partial
supraspinatus tear + LHB tenosynovitis |
5.7 → 3.2 |
7 → 3 |
−4 (−57 %) |
Quick-DASH: 86 → 2.3 (+97 %) |
Complete healing of supraspinatus tear; decreased LHB effusion; mild new subacromial-deltoid bursitis |
|
4 (M, 43) |
Right elbow – Partial enthesis lesion
of extensors (epicondylitis) |
5.0 → 2.8 |
6 → 1 |
−5 (−83 %) |
PRTEE: 57 → 1 (+98%) |
Complete restitutio ad integrum; new echogenic fibers at enthesis; normal periosteum |
|
5 (F, 64) |
Left knee – Partial LCL lesion + periosteal irregularities |
4.0 → 2.1 |
5 → 2 |
−3 (−60 %) |
KOOS: 52 → 100 (+92 %) |
Complete healing of LCL; resolution of periosteal
notches; bursitis resolved |
Table 1
Clinical, functional and ultrasound outcomes for the five patients treated with MLS® M-Hi laser therapy.
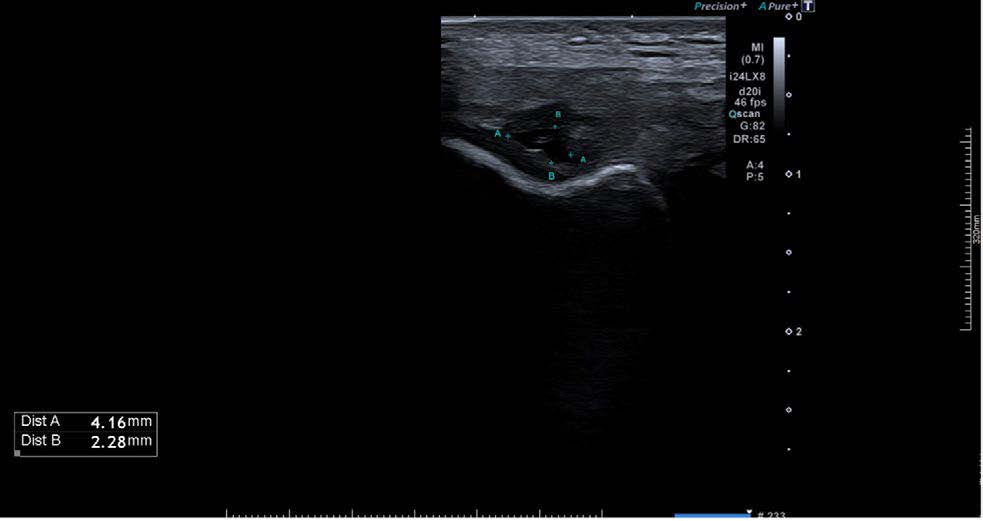

Figure 1
Longitudinal ultrasound images of the common extensor tendon enthesis at the lateral elbow.
(A) Baseline examination showing a focal anechoic area (~2 × 3 mm) at the tendon enthesis, consistent with a partial-thickness lesion and disruption of the normal fibrillar pattern.
(B) Post-treatment examination demonstrating resolution of the anechoic area and restoration of a homogeneous fibrillar architecture
Bibliography
- Chisari E, Rehak L, Khan WS, Maffulli N. Tendon healing is adversely affected by low-grade inflammation. J Orthop Surg Res. 2021;16:700. doi:10.1186/ s13018-021-02813-8.
- Malliaras P, Barton CJ, Reeves ND, Langberg H. Achilles and patellar tendinopathy loading programmes: mechanisms of effectiveness. Sports Med. 2013;43(4):267–286. doi:10.1007/ s40279-013-0019-z.
- Bjordal JM, Couppé C, Chow RT, Tuner J, Ljunggren EA. A systematic review of low-level laser therapy with location-specific doses for pain from chronic joint disorders. Photomed Laser Surg. 2006; 24(2):158–168. doi:10.1089/pho.2006.24.158.
- Draghi F, Gitto S, Bortolotto C, Draghi AG, Ori Belometti G. Imaging of the elbow: a pictorial review. Skeletal Radiol. 2013;42(6):789–800.doi:10.1007/ s00256-013-1604-5.
- Chow RT, Johnson MI, Lopes-Martins RAB, Bjordal JM. Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis. Lancet. 2009;374(9705): 1897–1908. doi:10.1016/S0140- 6736(09)61522-1.
- Leal Junior ECP, Lopes-Martins RAB, Bjordal JM. Effects of phototherapy (low-level laser therapy and light-emitting diode therapy) on delayed onset muscle soreness. Lasers Med Sci. 2010;25(2):231–236. doi:10.1007/s10103-009-0692-3.
- Tumilty S, Munn J, McDonough S, Hurley DA, Basford JR, Baxter GD. Low-level laser therapy combined with eccentric exercise for Achilles tendinopathy: a randomised controlled trial. Arch Phys Med Rehabil. 2010;91(8):1292–1298. doi:10.1016/j.apmr.2010.05.009.
- Stergioulas A. Low-level laser treatment combined with eccentric exercise for chronic Achilles tendinopathy. Photomed Laser Surg. 2008;26(2):99–105. doi:10.1089/pho.2007.2126.
- Lam LK, Cheing GLY. Effects of therapeutic laser on lateral epicondylalgia and patellar tendinopathy: an evidence-based practice approach. J Orthop Sports Phys Ther. 2007;37(4):223–229. doi:10.2519/jospt.2007.2430.
- Figen A, et al. Effects of photobiomodulation combined with exercise on lateral epicondylalgia: a clinical trial with ultrasound evaluation. Clin Rehabil. 2021.
- Genah-Monici F, et al. MLS® laser effects on fibroblast migration, collagen I synthesis, and cytokine modulation in wound-healing models. Energy Health. 2021;19(1):10–18.
- Monici M, Cialdai F, et al. Proteomic and cytoskeletal effects of infrared MLS® irradiation on myoblasts under altered gravitational conditions. Microgravity Sci Technol. 2012;24(4):249–262. doi:10.1007/s12217-012-9308-4.
- Gigo-Benato D, Geuna S, Rochkind S, et al. Effects of laser therapy on peripheral nerve regeneration after end-to-side neurorrhaphy. J Peripher Nerv Syst. 2004;9(4):240–250. doi:10.1111/ j.1085-9489.2004.09405.x.
- Micheli A, Monici M, et al. Effects of MLS® MiS laser therapy on neuropathic pain and myelin repair in chronic constriction injury models. Energy Health. 2019;17(2):22–30.