Energy for Health, Vol. 23, 2023
Liliya P. Panayotova1, Ilia T. Todorov2*
1Medical University of Varna, Department of Physiotherapy, Rehabilitation, Thalassotherapy and Occupational Diseases, Varna and St. Marina University Hospital of Varna, and 2Heart and Brain Hospital, Burgas, Bulgaria
*Corresponding author: Ilia T. Todorov, Clinic of Physical and Rehabilitation Medicine, Heart and Brain Hospital, 1 Zdrave Str, 8000, Burgas, Bulgaria. E-mail: [email protected]
Abstract
Objective: To evaluate the therapeutical effects of Multiwave Locked System (MLS®) laser and the combined therapy of microwave diathermy and interference current, in patients with glenohumeral joint peritendinitis.
Design: This was a prospective, randomised, parallel, single center trial.
Setting: Outpatient Hospital Clinic
PARTICIPANTS: A sample of 76 patients with glenohumeral joint peritendinitis
Methods: The patients were randomized into 2 groups in a 1:1 ratio: a group was treated with MLS® Laser Therapy (group A) and a group with microwave diathermy and interferential current therapy (group B). The primary outcome was the reduction of pain according to Shoulder Pain and Disability Index (SPADI). Secondary outcomes were improvements of shoulder’s movement (goniometry) and the reduction of pain, through the visual analogue scale (VAS). An intragroup and an intergroup analysis were performed.
Results: Both treatments demonstrated statistically significant intragroup differences. The intergroup analysis showed a greater improvement of MLS® Laser Therapy in terms of pain reduction at the end of the treatment and at the midterm follow-up visit.
Conclusion: Both therapies have been demonstrated to be effective and safe. The application of MLS® laser treatment presented more effective and durable therapeutic effects.
Lay Abstract
The purpose of the present investigation is to evaluate the therapeutical effects, in terms of pain reduction and mobility improvement, of Multiwave Locked System (MLS®) laser energy treatment and the combined therapy of microwave diathermy and interference current.
A total of 76 patients were recruited for the study. They were split into two groups: Group A received eight sessions of MLS® laser; Group B – 10 sessions of microwave diathermy and interferential current. All the patients were evaluated at baseline prior to starting treatment (T0), after completion of the therapeutic course (T1), and on the 45th day from baseline (T2). The intergroup analysis showed a greater improvement of MLS® Laser Therapy in terms of pain reduction at the end of the treatment and at the mid-term follow-up visit. It also presented more effective and durable therapeutic effects.
Introduction
Glenohumeral joint peritendinitis is one of the most common shoulder diseases [1, 2], that affects people who practice sports as well as repetitive activities related to work or to everyday life [3].
Moreover, peritendinitis of rotator cuff muscles aggravates with ageing [4] and affects more than 80% of the people over 80 years of age [5]. According to its definition, tendinitis suggests that tendon injury is accompanied by an inflammatory response [6-9].
The glenohumeral joint peritendinitis affects rotator cuff tendons, most commonly, of m. supraspinatus. This damage can vary from a simple tendinopathy to degenerative alterations, even to their partial or complete rupture. On the other hand, the glenohumeral joint peritendinitis very often leads to a secondary adhesive glenohumeral joint capsulitis (frozen shoulder), due to a pain-induced disturbed movement mechanism [10].
It appears as an evolution of an initially controlled inflammatory process, starting after a traumatic moment and evolving towards an abnormal uncontrolled fibrosis [11, 12]. Its origin should be considered a severe medical failure, as glenohumeral joint function is not always completely restored in some patients [13].
Approximately 40% of the rotator cuff tendinopathy patients fail to respond to conservative management [14,15] and more than one half of the patients report a reiterating and permanent pain in the long term [16]. The rotator cuff tendinopathy is widely common and represents a considerable socio-economic burden because of work loss and treatment costs [17].
Investigations on the effects of Multiwave Locked System (MLS®) lasers have shown the possibility to influence immediately the disease pathogenesis [18-25] and the opportunity to use the therapeutic lasers in any phase of disease stage. Such characteristics make the MLS® Laser Therapy a suitable application in the treatment of glenohumeral joint peritendinitis [13].
Therapeutic modalities, local microwave diathermy and interferential current are commonly used for the glenohumeral joint peritendinitis. They can help in the restriction of the degeneration processes through a restoration improvement [25] and a reduction of tissue neovascularization that is related to tendinopathy pathogenesis [6]. Diathermy exerts several biological effects such as metabolic function enhancement, deep tissue temperature elevation, and blood microcirculation improvement.
As a result, from these effects, pain reduces and joint movement volume increases. The contraindications for the usage of this modality include the application on metal [ 26], metabolic imbalance and pacemakers [14]. The therapy with interferential currents consists in the application of an alternating medium-frequency current (4000 Hz) modulated at a low frequency (0-250 Hz). One of the advantages of the interferential currents over the low-frequency ones consists in their capacity to penetrate into the human organism despite the skin resistance. Another advantage of the interferential current is its capacity to generate low frequency current in deep tissues in the area of treatment.
In the literature available, several theoretical physiological mechanisms such as the ‘gate control’ theory, enhanced circulation, pain reduction, nervous conductivity blockade and placebo have been proposed to support the analgesic effects of the interferential current [27,28].
Materials and Methods
This prospective, randomised, parallel, single centre trial was conducted at the St. Marina University Hospital of Varna. The scientific research has been conducted in accordance with the principles set forth in the Helsinki Declaration and received the permission from the Commission on Ethics of Scientific Research, appointed at the Medical University of Varna – protocol № 98 / 26.11.2020. Data were collected in a group of patients (n=76) with acute glenohumeral joint peritendinitis. The researchers have received permission from the hospital authority to conduct the trial in the hospital. All the enrolled subjects gave their consent to participate at the study and filled the informed consent.
Patients with the following conditions have been included: diagnosis of glenohumeral joint peritendinitis verified by means of a physical examination, clinical manifestations such as palpable pain in the projection of the insertions of the affected muscles, reduced joint active flexion, abduction and external rotation, no physical therapy and/or laser treatment during the period after pain onset.
Patients with the following conditions have been excluded: a diagnosed shoulder-complex bone fracture, a proved rupture of the tendon of m. supraspinatus or another tendon of the rotator cuff muscles and of m. biceps brachii, history of pain symptoms lasting longer than one week or chronically relapsing complaints in the affected shoulder, a consulting examination by orthopaedist requiring any surgical intervention, applications of corticosteroid preparations or other drugs after pain onset, any comorbidity creating contraindications for laser treatment such as systemic neoplastic, infectious and autoimmune diseases as well as for conventional physical therapy, a preceding surgical intervention in the affected shoulder, a fifth and sixth skin type after Fitzpatrick, an incapacity to understand and observe the study protocol, patients who refused to sign the informed consent concerning the therapeutic procedures, patients who refused to participate to the study due to personal reasons, a pregnancy state.
Аfter patients have passed an initial assessment of inclusion / exclusion criteria they were randomised into 1 of 2 groups in a 1:1 ratio. A group was treated with the MLS® Laser Therapy – group A – while the other with a combination of microwave diathermy and interferential current therapies – group B. The principal investigator generated the distribution sequence (by software platform GraphPad), enrolled the participants, and assigned participants to interventions (Figure 1).
Interventions
The MLS® is a type of near infrared class IV high power laser distinguished by two simultaneous emissions. The two types of laser sources emit radiations of different wavelengths, peak power and emission regime. The first one is a pulsed diode laser at 905 nm with a pulse duration of 100 ns and a peak power of 25 W. The second diode laser emits a radiation wavelength at 808 nm in a constant regime (max power 1W for each diode) or in “frequenced” regime with a repetition frequency up to 2000Hz and a fixed duty cycle of 50%.
The patented system of synchronized sources enables their combined application with a total average power up to 1.1W or 3.3W, depending on the laser applicator (heandpiece), a peak power of 25W, a modulation frequency of 1-2000 Hz or continuous.
The MLS® Laser Therapy device used in this study is M6 (ASA srl -Arcugnano, Italy), equipped with both a robotized multidiode head (up to 3,3W), able to perform automatic scanning treatments, and an MLS® handpiece (up to 1,1W), aimed to perform manual point to point or scanning treatments.
Each treatment included two stages: the scanning of the frontal and dorsal shoulder area of 93 cm2 each with a robotized multidiode head (Figure 2-1) and a point-by-point process with the manual handpiece with 7 points of 3,14 cm2 area each were treated (Figure 2-2), for a total area of 21,98 cm2.
The two different parameter settings used, based on the application mode, are reported in the Table I. The therapeutic plan included eight sessions divided within two working weeks. In the first week each patient underwent to a daily treatment for Randomisation procedure a total of five days and five procedures, while in the second week, a daily procedure was performed every second day for a total of three procedures.
The therapeutic method used in group B included ten sessions divided within two working weeks, every day each patient received one application of microwave electromagnetic field and one of interferential currents.
The microwave electromagnetic f ield (Figure 3-1) has been used with the following parameters setting: wavelength of 12,6 cm and frequency of 2375 MHz, microwave intensity of 0,56 W/cm2, power of 40-70 W or less, session duration of 10-15 minutes and subjective dosage – athermic with gradual increase up to oligothermic that is felt as a very slight heat. For the interferential currents (Figure 3-2) has been used a four-pole method with the following parameters: alternating current, sinusoid impulse, bearing frequency of 4000 Hz, alternating frequency of 90-100 Hz, session duration of 15 min and subjective dosage – up to the sensation of running current.
Sample Size Calculation
A convenient sample of patients with peritendinitis of glenohumeral joint participated in this study.
The relationship between significance, power, sample size and effect size is used to make sample size calculation. To avoid Type II error, or false negatives it is generally accepted we should aim for a power of 0,8. Our calculations were made using a significance level alpha = 0.05 and the test has 80% power, and if assumed a medium effect size of 0.5, it is needed a sample size of about 32 patients in each group. A total of 76 patients fulfilled the inclusion criteria and were enrolled in the study.
Randomisation Procedure
All enrolled subjects were randomly allocated either to group A or B using online generated sequence for random distribution (1:1). The software platform used was GraphPad (https://www.graphpad.com/quickcalcs/randomize1.cfm).
It randomly scrambles a set number of participants among a set number of treatment slots, so each treatment always gets assigned the same number of participants. The random allocation sequence has been created by the leading author – Dr. Panayotova. She was also responsible for the enrollment of the participants and for the procedure assignment.
Primary Outcome Measures
For evaluation of the functional status and of pain during the follow-up we used the Shoulder Pain and Disability Index (SPADI). It is a self-administered questionnaire that consists of two dimensions, one for pain and the other for functional activities. The pain dimension consists of f ive questions regarding the severity of an individual‘s pain. Functional activities are assessed with eight questions designed to measure the degree of difficulty an individual has with various activities of daily living that require upper-extremity use.
The patient is asked to circle the number from 0 to10 scale that best describes the pain or disability. The total score is measured as a percentage and is equal to the sum of points collected from all answers to the 13 questions divided by the maximum number of 130 points multiplied by 100. The means of the two subscales are averaged to produce a total score ranging from 0 (best) to 100 (worst). Minimum Detectable Change (90% confidence) = 13 points (29). All the patients were evaluated in three different moments: at baseline prior to starting treatment (T0), after completion of the therapeutic course (T1), and on the 45th day from baseline (T2).
Second Outcome Measures
In order to objectify the functional improvement an anglemetry of glenohumeral joint has been used. An eventual increase of range of motion (ROM) corresponds to the patient’s improvement. The movements evaluated were: flexion (F), abduction (Abd) and external rotation (ER), (Figure 4). Other parameters included in the study were the assessment of spontaneous and palpable pain, according to the visual analogue scale (VAS_s, VAS_p). This is a measuring instrument that attempts to measure a characteristic or relationship that is considered not to be easily measurable directly. (30) VAS is a straight horizontal line with a fixed length, usually 100 mm. The patient notes the degree of spontaneous pain (no movement in the affected joint) and pain on palpation in the projection of the insertion of m. infraspinatus. When reporting the results for every 10 mm of the line correspond to the following points and levels of pain: 0 – no pain, 1-2 – mild pain, 3-4 – moderate pain, 5-6 – severe pain, 7-8 – a lot severe pain, 9-10 – unbearable pain. A minimum clinically important difference of 1.37 cm has been determined for a 10-cm pain VAS in patients with rotator cuff disease evaluated after 6 weeks of nonoperative treatment. (31) As a palpation spot we chose, due to its high recurrence rate, the insertion of the supraspinatus muscle. For that the greater tubercule of the humerus has to be identified and the palpation pressure should be applied to its proximal – lateral – anterior aspect. The patients were evaluated in three different moments: at baseline prior to starting treatment (T0), after completion of the therapeutic course (T1), and on the 45th day from baseline (T2).
Statistical Methods
Continuous variables are summarized as mean ± SD, and categorical variables are reported as frequencies or percentages. The Shapiro-Wilk test was used to analyse the normal distribution of the variables. Continuous variables were compared using Student t tests or Wilcoxon rank sum tests if the data were not normally distributed. Categorical variables were compared using chi-square tests or Fisher exact tests if >25% of the cells in the contingency table had expected frequencies <5. A p value <0.05 was considered to indicate statistical significance for all analyses. Cohen’s D (standardized mean difference) was used. This is one of the most common ways to measure effect size.
Two statistical analyses were performed: an intragroup analysis, to evaluate, for both therapeutic methods, the differences of each parameter in the three different evaluation moments and an intergroup analysis, to compare the outcomes obtained through the two different therapeutic methods.
In the intragroup analysis Friedman’s and Wilcoxon’s nonparametric tests and the paired T-test have been run, while in the intergroup analysis the Mann-Whitney’s nonparametric test was used.
Statistical analyses were performed using SPSS software.
Results
A total of 78 patients were enrolled between November 2020 and September 2021. After patients have passed an initial assessment of inclusion / exclusion criteria 76 of them were randomised by software platform either to the MLS® group (n=38) or to the microwave electromagnetic field and interference currents group (n=38). 2 of the patients have been excluded due to not meeting the inclusion criteria.
All the enrolled patients completed the 45th day follow-up visit. Baseline data were obtained for all the patients. The average age at baseline was 45.7±10.2 years, and 52.6% were men. In the 60.5% of the cases was treated the right shoulder. At baseline, the difference from the normal of the anglemetry of humeral joint was 28°±24° for the flexion, 32°±27° for abduction and 34°±27° for external rotation. The baseline value spontaneous VAS was 3.1±2.8, palpatory VAS was 4.8±2.0 and SPADI was 57.4%±22.6%. There were no differences in the demographic, physical and pain evaluation between the 2 groups thus resulting homogeneous each other (Table II).
In Table III are reported the results of the intragroup statistical analysis. As shown, for the patients treated with the MLS® Laser Therapy, a significant difference of the mean values calculated in correspondence of the three time points have been found in the humeral joint movement analysis (Figure 5) – flexion, abduction and external rotation – and in the pain and functional evaluation analysis – VAS and SPADI scores. Such improvement trend is significant even at the mid-term follow-up visit. Only the differences concerning the spontaneous pain, according to VAS, between T1 and T2 values, resulted not statistically different (p-value = 0,058) (Figure 5). It is reasonable to consider this aspect related to the great initial improvement the patients achieved after the treatment cycle completion, the low initial VAS_s value (2.8 ± 3.0 cm) and the marginal improvement obtained at follow-up.
For the patient treated with microwave electromagnetic field and interferential currents (MW_IT), there is a statistically significant difference in the mean values of the palpatory and spontaneous pain according to VAS, as well as in the percentage SPADI scores (Figure 5). As a consequence of chance, the differences between After and D45th scores were found for humeral joint flexion (p-value = 0,658), abduction (p-value = 0,285) and external rotation (p-value = 0,166) (Figure 5). This is due to the fact that these patients achieved a maximal and long-lasting improvement after treatment completion, too. In the cases of statistically significant differences between the T1 and T2 mean values confirm a trend of improvement that continue even after the end of the treatment cycle.
The intergroup analysis results are reported in Table IV and represented in Figure 6. The two groups have been compared at the end of the treatment cycle and at the follow-up. One half of the parameters present a statistically significant difference of the mean values in favour of the treatment method used in laser MLS® group (A). After treatment completion, MLS® Laser Therapy group resulted statistically different from the MW_IT group (B) in terms of: spontaneous pain (0.6cm vs 1.1cm, p = 0.016), palpatory pain (2.2cm vs 3.7cm, p < 0.000) and SPADI score (23.5% vs 35.9%, p-value = 0.003); a greater improvement seems achievable through the MLS® Laser Therapy. The two groups result not statistically different in terms of improvement of ROM of the glenohumeral joint movements.
At the mid-term follow-up visit, 45 days after the beginning of the therof motion in comparison to other physical agents. apy, it is reported a significant difference between the two groups in favour of the MLS® treatment group in terms of shoulder flexion (5.9° vs. 8.29°, p = 0.009), palpatory pain according to VAS (1.1cm vs. 3.2cm, p < 0.000) and percentage SPADI scores (17.6% vs. 31.4%, p < 0.000).
Cohen’s D, or standardized mean difference, is one of the most common ways to measure estimated effect size. The measurement estimated effect size was used if the data were normally distributed (SPADI and VAS_p). Standardized mean difference is as follows: VAS_p T0 Group A 0.87, VAS_p T1 Group A 1,52, VAS_p T2 Group A 0,79, VAS_p T0 Group B 0.81, VAS_p T1 Group B 0.86, VAS_p T2 Group B 0,37, SPADI T0 Group A 1,61, VSPADI T1 Group A 1,65, SPADI T2 Group A 0,65, SPADI T0 Group B 1.82, SPADI T1 Group B 1.62, SPADI T2 Group B 0,33.
Discussion
The findings of our study showed a statistically significant decrease in pain and an improvement of the shoulder functionality with both therapeutic methods. MLS® laser group demonstrated to be superior in reducing palpatory pain according to VAS scale and percentage of disability according to SPADI, and showed similar improvement in ROM compared to the combined microwave diathermy and interference current group.
Our results are in accordance with Eslamian et al 2012 (32) where a LLLT at 830nm was applied with similar dosage (4J/cm2) and combined with conventional physiotherapy demonstrating superiority over routine physiotherapy from the view of decreasing pain and improving the patient’s function, but no additional advantages were detected in increasing shoulder joint range of motion in comparison to other physical agents.
A recent systematic review including 11 studies and involving 486 participants (33), report that the results of using LLLT to improve pain and function in shoulder tendinopathies are controversial. Only 45% of the 11 studies included showed a statistically significant decrease in pain; and only 1 of the 6 studies that assessed functional outcomes observed a statistically significant improvement. However, the results obtained in our study with the application of MLS® Laser Therapy seem to strengthen the evidence in favor of laser therapy in improving function and ROM as well as pain. This could depend on the characteristics of the laser emission and the setting dose applied in our study.
This hypothesis seems to be conf irmed by another systematic review with meta-analysis based on 17 randomized controlled trials (RCTs) focused on LLLT treatment effects in shoulder tendinopathy (34). This review underlined that trials performed with inadequate laser doses were ineffective across all outcome measures. The same review confirms that adequate laser doses (according to WALT guidelines) can offer clinically relevant pain relief both alone and in combination with physiotherapy interventions, while secondary outcome measures of shoulder function were only significantly in favor of LLLT when used as monotherapy.
On the other hand, the strong biological effects of the MLS®: anti-inflammatory, anti–oedema and analgesic, have been explained at a cellular level by Monici and team in a proteomic study published in 2013.(35) It was conducted on muscle cells (myoblasts) and has proven that MLS® treatment induces an increase of anti-inflammatory protein NLRP 10. That protein inhibits the activity of caspase-1 and the protein complex PYCARD, which promotes the maturation of the inflammatory cytokines interleukin-1 β (IL-1β) and interleukin 18 (IL-18). Therefore, in turn, NLPR 10 inhibits the production of pro-inflammatory interleukins IL-1β and IL-18, reducing inflammation.
These evidences support our findings that MLS® Laser Therapy, used as monotherapy, is an effective tool for reducing pain and improving overall function.
Previous investigations on the effect of MLS® lasers have shown the possibility to influence immediately the disease pathogenesis and to be applied in any phase of the disease stage. This suggests an early use of the MLS® Laser Therapy as primary option in comparison with conventional physical therapy. The latter is associated with higher therapeutical risks, especially when applied in the early stage of the disease. Investigations on the effects of MLS® Laser Therapy applied with different settings (frequency, power, dosage) on this disease, as well as the comparison of MLS® laser with other common physical factors, could be of further interest. According to our clinical practice, including the research work, all the tender / trigger palpation points could be eliminated in up to 3 sessions which is an excellent demonstration of the analgesic effect of the MLS®. The effect manifests within seconds of treatment and even if a recurrence of the tender / trigger point is sometimes observed, if treated for a second time it is permanently resolved.
With the exception of patients contraindicated or at risk for treatment with laser therapy or with microwave diathermy and interferential current, with due precautions the potential side effects and harms to study participants are minimal. Unintended effects in each group such as exacerbation of existing pain symptoms, headache and dizziness may occur, and they are a manifestation of individual intolerance to the microwave diathermy. [36] During the course of the study, no severe adverse events have been observed in both groups. Regardless of the initial pain intensity and ROM limitation, both treatment protocols resulted well tolerated by the patients.
Despite the current scientific research publications [13, 18, 37-40], further researches on the MLS® Laser Therapy in glenohumeral joint peritendinitis patients are desirable. A limit of the current study is that it is not blinded and further studies comparing sham and real MLS® Laser Therapy could better prove the therapeutic effects of laser treatment. Another limitation is the 45 days follow–up as in the clinical practice the glenohumeral peritendinitis is known as a disease with high recurrence percentage. A three or even six months follow – up will provide a better reference to that matter.
Conclusion
Our clinical experience supports the conclusion that both therapeutic methods used – MLS® laser treatment and combined physical complex of microwave diathermy and interferential current – are suitable as a common protocol for routine clinical practice in the patients with glenohumeral joint peritendinitis.
Both treatments have shown to improve the joint movement and to reduce the pain, and in both groups no adverse events happened during the course of the study. In particular, one half of the registered clinical parameters presented a statistically significant difference of the mean values in favour of the treatment method used in laser therapy group (A). The application of the MLS® Laser Therapy treatment enabled a successful and long-lasting influence on these patients. The applicability of the method depends on the personnel training and the availability of an MLS® laser device. This modern monotherapy option needs to be further evaluated but it can be considered a valid alternative to any other combined double or triple physical therapies.
Bibliography
- van der Windt DA, Koes BW, de Jong BA, Bouter LM. Shoulder disorders in general practice: incidence, patient characteristics, and management. Ann Rheum Dis. 1995;54(12):959-964.
- Vecchio P, Kavanagh R, Hazleman BL, King RH. Shoulder pain in a community-based rheumatology clinic. Br J Rheumatol. 1995;34(5):440-442.
- Cools AM, Declerq G, Cagnie B, Cambier D, Witvrouw E. Internal impingement in tennis player: rehabilitation guidelines. Br J Sports Med. 2008;42(3):165-171.
- Tempelhof S, Rupp S, Seil R. Age-related prevalence of rotator cuff tears in asymptomatic shoulders. J Shoulder Elbow Surg. 1999;8(4):296-199.
- Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M. Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender. J Bone Joint Surg Br. 1995;77(2):296298.
- Aicale R, Tarantino D, Maffulli N. Overuse injuries in sport: a comprehensive overview. J Orthop Surg Res. 2018 Dec 05;13(1):309.
- Andres BM, Murrel GA. Treatment of tendinopathy: what works, what does not, and what is on the horizon. Clin Orthop Rel Res. 2008;466(7):1539-1554.
- Lädermann A, Cunningham G, Chagué S, Charbonnier C. Sexual Activities as Risk Factors of Rotator Cuff Lesions: A Prospective Cohort Study. Sex Disabil. 2018;36(4):305-311.
- Spargoli G. SUPRASPINATUS TENDON PATHOMECHANICS: A CURRENT CONCEPTS REVIEW. Int J Sports Phys Ther. 2018 Dec;13(6):1083-1094.
- Debruner H, Hep V. Orthopedic diagnostics. Sofia: Medicina i fizkultura; 1996.; 113- 126.
- Todorov I. The syndrome of the “frozen” shoulder – features and modern therapeutic approach, Universitetsko izdatelstvo MU-Varna, 2014.
- Kabbabe B, Ramkumar S, Richardson M. Cytogenetic analysis of the pathology of the frozen shoulder. Int J Shoulder Surg, 2010; 4(3):75-78.
- Smiderle C, Scapin M: MLS® therapy treatment of acute shoulder pain in inflammatory processes of the rotator cuff, Energy For Health, 1: 12 – 15, 2004.
- Brox JI, Gjengedal E, Uppheim G, Bohmer AS, Brevik JI, Ljunggren AE, et al. Arthroscopic surgery versus supervised exercises in patients with rotator cuff disease (stage II impingement syndrome): a prospective, randomized, controlled study in 125 patients with a 2 1/2-year followup. J Shoulder Elbow Surg 1999; 8: 102–111.
- Holmgren T, Bjornsson Hallgren H, Oberg B, Adolfsson L, Johansson K. Effect of specific exercise strategy on need for surgery in patients with subacromial impingement syndrome: randomised controlled study. BMJ 2012; 344: e787.
- Winters JC, Sobel JS, Groenier KH, Arendzen JH, Meyboomde Jong B. The long-term course of shoulder complaints: a prospective study in general practice. Rheumatology (Oxford) 1999; 38: 160–163.
- Smith KL, Harryman DT 2nd, Antoniou J, Campbell B, Sidles JA, Matsen FA 3rd. A prospective, multipractice study of shoulder function and health status in patients with documented rotator cuff tears. J Shoulder Elbow Surg. 2000;9(5):395-402. doi:10.1067/ mse.2000.108962.
- Corti L., MLS® Laser Therapy treatment of shoulder pain: a controlled comparative study Scientific Report MLS®, 2004.
- Caruso G, Gervasi S, Salvadori D: Physical treatment of post-traumatic gonalgia by NIR laser therapy: a case report, Energy For Health, 9: 15 – 17, 2012.
- Corti L, Rosa E, et all.: Clinical results in the treatment of ankle and knee distortion pathologies with MLS® therapy, Energy For Health, 1: 30 – 34, 2004.
- Iacopetti I, Perazzi A, et al.: Effect of MLS® Laser Therapy with different dose regimes for the treatment of experimentally induced tendinopathy in sheep: pilot study, Photomed Laser Surg, 33 (3): 154 – 163, 2015.
- Pasternak-Mnich K, Wróbel D, Nowacka O, Pieszyński I, Bryszewska M, Kujawa J. The effect of MLS® laser radiation on cell lipid membrane. Ann Agric Environ Med. 2018; 25(1): 108–113. doi: 10.5604/12321966.1230734.
- Rioja Toro J, Estevez Poy Pj, Martinez Padro F. A prospective, randomized and placebo-controlled study of the efficacy of treatment with laser, with or without splinting of wrist in idiopathic carpal tunnel syndrome, Rehabilitacion (Madr), 46 (2): 92 – 102, 2012.
- Tasca A. MLS® therapy treatment of various osteo / muscular / tendinois pathologies, Scientific Report MLS®, 2004.
- Viliani T. Laserpuncture with MLS® (Multiwave Locked System) System Mphi: safety and clinical efficacy in joint disease, preliminary data, Energy For Health, 13: 4 – 8, 2014.
- Draper DO, Castel JC, Castel D. Low-watt pulsed shortwave diathermy and metal-plate fixation of the elbow. ATT. 2004;9(5):2832.
- Palmer S, Martin D. Interferential current for pain control. In: Kitchen S ed. Electrotherapy Evidence-based Practice. 11th ed.Edinburgh, Scotland: Churchill Livingstone; 2002:287–298.
- Low J, Reed A. Electrical stimulation of nerve and muscle. In: Low JReed A eds. Electrotherapy Explained: Principles and Practice. 3rd ed.Oxford, United Kingdom: Buttherworth-Heinemann; 2000:43–140.
- Roach KE, Budiman-Mak E, Songsiridej N, Lertratanakul Y. Development of a shoulder pain and disability index. Arthritis Care Res. 1991 Dec;4(4):143-9.
- D. Gould et al. Visual Analogue Scale (VAS). Journal of Clinical Nursing 2001; 10:697-706
- Joyce CR, Zutshi DW, Hrubes V, Mason RM. Comparison of fixed interval and visual analogue scales for rating chronic pain. European journal of clinical pharmacology. 1975 Nov;8(6):415-20.
- Eslamian F, Shakouri SK, Ghojazadeh M. et al. Effects of low-level laser therapy in combination with physiotherapy in the management of rotator cuff tendinitis. Lasers Med Sci 27, 951–958 (2012).
- Leotty CLR, Lima MMC, Araújo FX. Effect of low-level laser therapy on pain and function of patients with shoulder tendinopathy: A systematic review. Fisioterapia e Pesquisa, 2020, 27: 210-217.
- Haslerud S. et al. The efficacy of Low-Level laser therapy for shoulder tendinopathy: a systematic review and Meta‐Analysis of randomized controlled trials. Physiotherapy Research International, 2015, 20.2: 108-125.
- Monici M, Cialdai F, Ranaldi F, Paoli P, Boscaro F, Moneti G, Caselli A. Effect of IR laser on myoblasts: a proteomic study. MOLECULAR BIOSYSTEMS, vol. 9, p.1147-1161, 2013. doi:10.1039/ C2MB25398D.
- Kostadinov D,Gacheva Y, Manual of physical therapy. Volume 1, Sofia: Medicina i fizkultura; 1989; 101.
- Vignali L, Caruso G, Gervasi S, Cialdai F. MLS® Laser Therapy in the treatment of patients affected by Tendinopathies, Energy for Health [16], 2017.
- Sirbu E, Onofrei R, Hoinoiu T, Petroman R. The Short-Term Outcomes of Multiwave Locked System (MLS®) Laser Therapy versus a Combination of Transcutaneous Nerve Stimulation and Ultrasound Treatment for Subacromial Pain Syndrome, Applied Sciences, 11, 2273, 2021.
- M, D’Angelo G. Laser therapy in the management of neuropathic pain: preliminary experience on 43 patients. Energy for Health [19], 2019.
- Pekyavas NO, Baltaci G. Short-termeffects of high-intensity laser therapy, manual therapy, and Kinesio taping in patients with subacromial impingement syndrome. Lasers in Medical Science, 2016.
Notes
Conflicts of Interest: The authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript. The authors report no involvement in the research by the sponsor that could have influenced the outcome of this work.
Authors’ Contributions: All authors contributed equally to the manuscript and have read and approved the final version of the manuscript.
| Application Mode | Frequency (Hz) | Intensity (%) | Mean Power (w) | Total Area (cm2) | Time (Min) | Energy (J) | Energy Dose (J/cm2) |
|---|---|---|---|---|---|---|---|
|
Scanning – Robotized multi-diode head |
700 |
50 |
~1 |
186 |
8 |
480 |
2.57 |
|
Point-by-Point – Manual handpiece |
700 |
50 |
0.3 |
21.98 |
8 |
144 |
6.56 |
Table 1
MLS® therapy protocol used.
| Variable | Group A - Laser MLS® (n=38) | Group B - MW_IT (n=38) | p-Value | |
|---|---|---|---|---|
|
Age (yrs) |
|
48 ± 8.10 |
43.5 ± 11.55 |
NS |
|
Male |
|
19 (53) |
21 (58) |
NS |
|
Shoulder-Side: Right |
|
22 (61) |
24 (66) |
NS |
|
Anglemetry of Humeral Joint (°) |
||||
|
|
Flexion |
30 ± 26.6 |
26.5 ± 22.6 |
NS |
|
|
Abduction |
38.7 ± 33.2 |
26.3 ± 18.7 |
NS |
|
|
External Rotation |
39.7 ± 28.0 |
28.7 ± 26.4 |
NS |
|
Pain – Visual Analogue Scale (mm) |
||||
|
|
VAS_spontaneous |
2.8 ± 3.0 |
3.4 ± 2.6 |
NS |
|
|
VAS_palpatory |
4.5 ± 1.8 |
5.1 ± 2.2 |
NS |
|
|
SPADI (%) |
49.2 ± 20.8 |
65.5 ± 21.5 |
NS |
|
Values are mean ± standard deviation (SD) or n (%) |
||||
Table 2
Demographic, physical and pain variables at Baseline.

Figure 1.1
CONSORT flow diagram


Figure 2
Group A – MLS® M6 laser therapy application treatment: (2.1) robotized scanning mode, (2.2) manual point-by-point headpiece mode.


Figure 3
Group B – combination of microwave electromagnetic field (3.1) and interference currents (3.2).
| Group A - Laser MLS | P-Value | Group B - MW_IT | p-value | |
|---|---|---|---|---|
| VARIABLES | Mean (SD) ; Min-Max |
T1-T0 T2-T1 T2-T0 |
Mean (SD) ; Min-Max |
T1-T0 T2-T1 T2-T0 |
| Flexion (in degrees) | ||||
| T0 | 30 (27) ; 0-100 | 0,000 | 26.5 (22) ; 0-90 | 0,000 |
| T1 | 9.3 (22) ; 0-90 | 0,003 | 8.7 (13) ; 0-70 | 0,658 |
| T2 | 5.92 (17) ; 0-70 | 0,000 | 8.3 (13) ; 0-70 | 0,000 |
| Abduction (in degrees) | ||||
| T0 | 38.7 (33) ; 10-150 | 0,000 | 26.3 (19) ; 10-100 | 0,000 |
| T1 | 12.6 (25) ; 0-110 | 0,007 | 8.2 (12) ; 0-60 | 0,285 |
| T2 | 7.8 (19) ; 0-80 | 0,000 | 7.1 (13) ; 0-60 | 0,000 |
| External Rotation (in degrees) | ||||
| T0 | 39.7 (28) ; 0-90 | 0,000 | 28.7 (26) ; 0-90 | 0,000 |
| T1 | 12.8 (22) ; 0-80 | 0,020 | 11.3 (20) ; 0-75 | 0,166 |
| T2 | 8.8 (18) ; 0-60 | 0,000 | 7.1 (13) ; 0-60 | 0,000 |
| VAS_spontaneous (cm) | ||||
| T0 | 2.8 (3) ; 0-10 | 0,000 | 3.4 (3) ; 0-10 | 0,000 |
| T1 | 0.61 (2) ; 0-8 | 0,058 | 1.1 (1) ; 0-6 | 0,002 |
| T2 | 0.26 (1) ; 0-5 | 0,000 | 0.7 (1) ; 0-5 | 0,000 |
| VAS_palpatory (cm) | ||||
| T0 | 4.5 (2) ; 0-7 | 0,000 | 5.1 (2) ; 0-10 | 0,000 |
| T1 | 2.2 (2) ; 0-10 | 0,000 | 3.7 (2) ; 0-7 | 0,014 |
| T2 | 1.1 (1) ; 0-5 | 0,000 | 3.2 (2) ; 0-7 | 0,000 |
| SPADI (%) | ||||
| T0 | 49.2 (21) ; 12-94 | 0,000 | 65.5 (22) ; 11-99 | 0,000 |
| T1 | 23.5 (21) ; 1-78 | 0,000 | 35.9 (19) ; 3-69 | 0,000 |
| T2 | 17.6 (18) ; 0-70 | 0,000 | 31.4 (21) ; 0-70 | 0,050 |
Table 3
Intra-group statistical analysis of the assessment indicators used in both groups at Baseline (T0), at the end of the treatment cycle (T1) and at the follow-up visit, 45 days since the beginning of the treatment (T2).
| Group A - Laser MLS | Group B - MW_IT | ||
|---|---|---|---|
| Variable | Mean (SD) | Mean (SD) | p-Value |
| Flexion (in degrees) | |||
| T1 | 9.3 (22) ; 0-90 | 8.7 (13) ; 0-70 | 0,658 |
| T2 | 5.92 (17) ; 0-70 | 8.3 (13) ; 0-70 | 0,000 |
| Abduction (in degrees) | |||
| T1 | 12.6 (25) ; 0-110 | 8.2 (12) ; 0-60 | 0,285 |
| T2 | 7.8 (19) ; 0-80 | 7.1 (13) ; 0-60 | 0,000 |
| External Rotation (in degrees) | |||
| T1 | 12.8 (22) ; 0-80 | 11.3 (20) ; 0-75 | 0,166 |
| T2 | 8.8 (18) ; 0-60 | 7.1 (13) ; 0-60 | 0,000 |
| VAS_spontaneous (cm) | |||
| T1 | 0.61 (2) ; 0-8 | 1.1 (1) ; 0-6 | 0,002 |
| T2 | 0.26 (1) ; 0-5 | 0.7 (1) ; 0-5 | 0,000 |
| VAS_palpatory (cm) | |||
| T1 | 2.2 (2) ; 0-10 | 3.7 (2) ; 0-7 | 0,014 |
| T2 | 1.1 (1) ; 0-5 | 3.2 (2) ; 0-7 | 0,000 |
| SPADI (%) | |||
| T1 | 23.5 (21) ; 1-78 | 35.9 (19) ; 3-69 | 0,000 |
| T2 | 17.6 (18) ; 0-70 | 31.4 (21) ; 0-70 | 0,050 |
Table 4
Inter-group statistical analysis of the assessment indicators used in both groups at Baseline, at the end of the treatment and at the follow-up visit, 45 days since the treatment start.

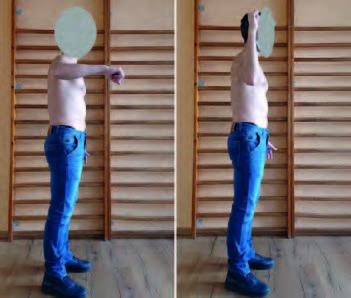

Figure 4
Evaluation of Aglemetry of humeral joint flexion, abduction and external rotation.
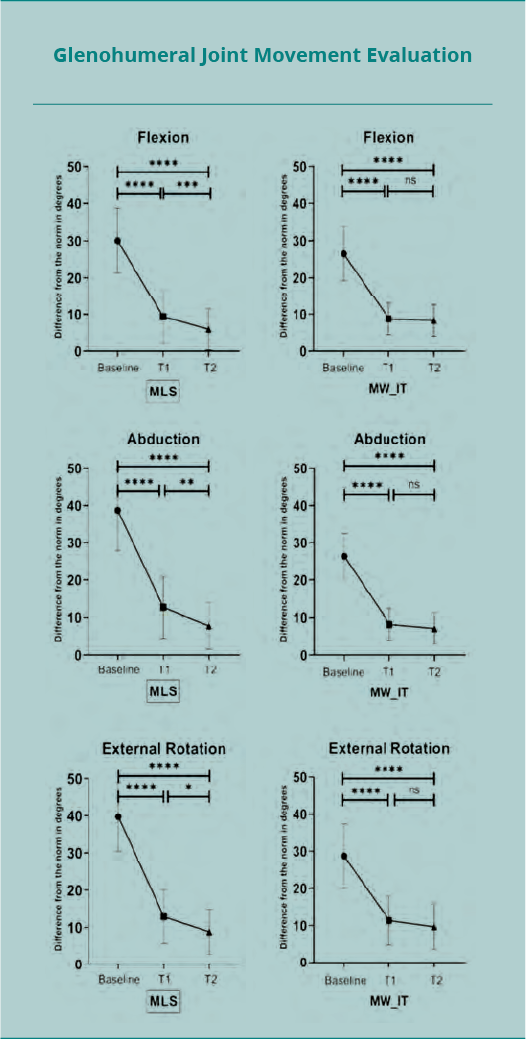

Figure 5
Mean values with 95% confidence interval (CI) of the clinical parameters evaluated at Baseline, in correspondence of the last treatment (T1) and after 45 days since the first treatment (T2) – difference from the normal of the glenohumeral Flexion, Abduction and External Rotation – assessment of spontaneous and palpatory pain according to the visual analog scale (VAS_s, VAS_p) and of functional status and pain through the Shoulder Pain and Disability Index (SPADI).
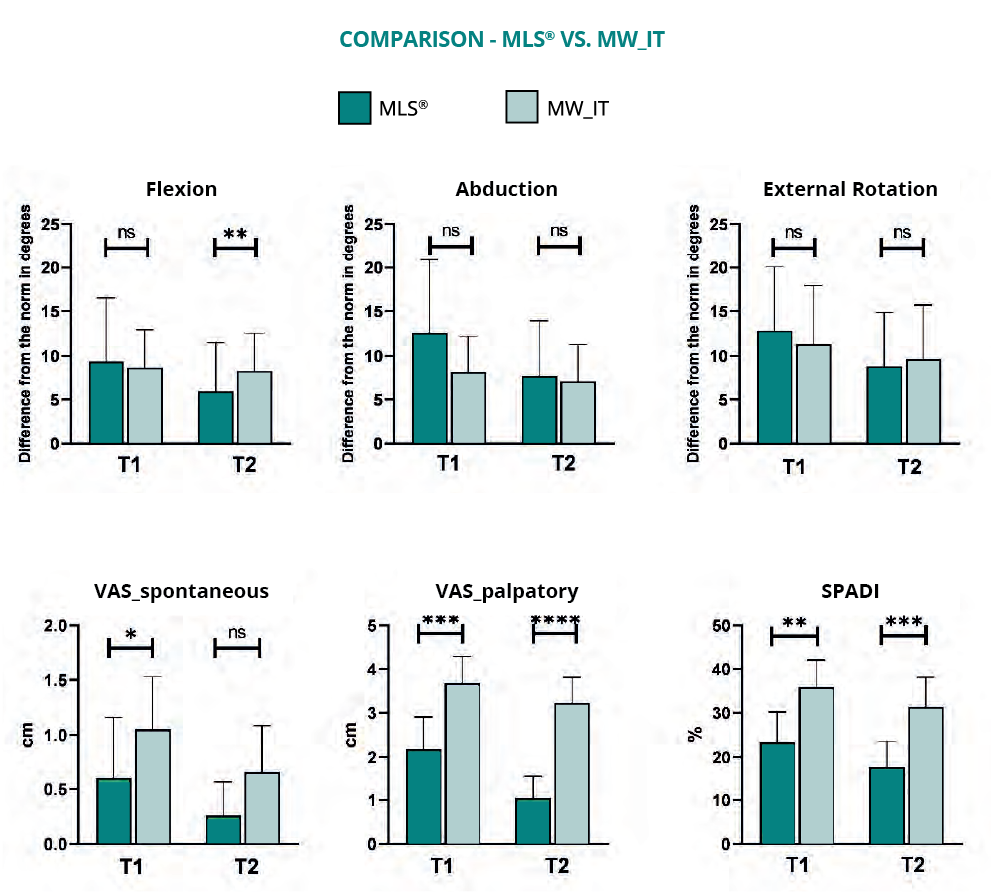
Figure 6
Mean values with 95% confidence interval (CI) of the clinical parameters and comparison between the two groups


