Case Report
In August 2022, a 69-year-old woman with a history of varicose eczema, diabetes, and chronic psoriasis, along with dermatological and arthritic manifestations, visited The Hills Foot Clinic due to a chronic venous ulcer on her left medial lower leg.
The patient reported limited mobility and the need for a walker or cane to ambulate.
From November 2021, the ulcer was managed by a home nurse who changed the dressings once a week. However, it gradually worsened until February 2022 when the patient was hospitalized. Cultural tests revealed a Pseudomonas aeruginosa infection. The patient received intravenous antibiotic therapy and local antiseptic dressings. After a week, the patient was discharged, and bi-weekly dress changes and medication were prescribed.
Despite undergoing new treatment therapy, the patient’s ulcer condition did not improve over the following six months. In fact, the pain worsened and became increasingly difficult to manage, necessitating the use of opioid oxycodone (Endone). This medication severely impacted the patient’s daily life, as it interfered with her ability to sleep and concentrate.
In patient’s words: “The home nurse came but the ulcers gradually got worse. I had to go to hospital. They put me on intravenous antibiotics. After seven days I returned home and then the wound clinic nurse came twice a week to dress them and treat them. They put heavy compression stockings on, and my ulcers got worse. I was crying with the pain and the frustration. I couldn’t do anything. I’ve got animals. I would feed the animals, take the Endone, wait for it to kick in and then come inside and just put my legs up. I had no help. I’m on my own.”
Standard therapy (debridement, medication, and dressing) was combined with MLS® laser treatment to reduce pain and promote healing. The laser treatment was initially applied every other day, for the first 4 weeks. Due to visible signs of healing, the treatment was then reduced to once a week for a total of 10 treatment sessions over 48 days.

Example of the MPhi 5 multidiode head in action during a laser treatment session. The red light 635nm-68nm is used as a pointer, it has a maximum power of 1 mW and no therapeutic effects
The multi diode head was used to apply laser treatment at approximately 20 cm from the skin (Figure 1). This was done after removing necrotic tissue and before administering medication and dressing. Both the patient and the doctor wore appropriate laser safety goggles. During each session was treated the ulcer’s area and the surround tissues. The device parameters were set as reported in Table 1.
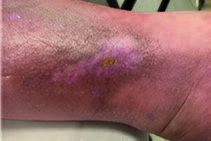
During the initial treatment visit on August 18th, 2022, the ulcer presented an area of approximately 15 cm2 (3 cm x 5 cm) – Figure 2.1. By the end of the visit, the patient reported a significant reduction in pain, which allowed her to discontinue the use of Endone. The analgesic effect was sustained throughout the treatment cycle, enabling the patient to cease taking opioids.
During treatment, the wound showed improvement with a progressive reduction in the superficial area, formation of granulation tissue, and reduction of exudate. The surrounding tissue inflammation also improved as the oedema gradually disappeared (see Figure 2.2-2.6). By the fifth visit, the ulcer area had reduced by more than 50% (2cm x 1cm).
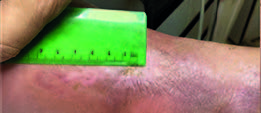
During the seventh visit, the patient reported a small trauma in the ulcer area, which appeared to have regressed. During a dressing change, green exudate was noticed. Due to discoloration at the edges of the ulcer, a recurrence of infection was suspected. The patient was sent to a general practitioner who prescribed a swab and preventive antibiotic treatment with Ciprofloxacin. After 5 days, the swab analysis showed no signs of infection, and the antibiotic therapy was stopped.
At the 9th MLS® laser treatment, the remaining wound appeared significantly smaller, with a superficial area of approximately 0.45 cm2 (0.9 cm x 0.5 cm) – Figure 2.9. After 48days and 10 MLS® laser treatments, the ulcer had closed, the quality of the surrounding tissue improved and there was no oedema.
The patient was discharged with the only prescription to wear an elasticated tubular bandage for mild compression and protection of the fragile new skin. No side effects were reported, and the satisfaction of the patient was high.
Patient said: “Look, for me, it was a miracle. I could not believe it. The ulcer is now totally fine. It is all clear. It was worth it. I’d do anything to get out of that pain. I could not stand it”.



Ulcer condition before removing necrotic tissue.

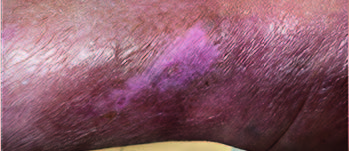
Ulcer condition after debridement and 3rd MLS® laser treatment.

The ulcer present depth reduced and eschar lifting with minimal scarring and surrounding skin much improved with significant reduction in leg’s oedema.

In occasion of the 5th visit the ulcer appear with a granulating base, no exudate, and a superficial area of ~ 2cm2.

Application of the MLS® laser during the 6th treatment, detain on the spacer used to maintain 20 cm distance from the skin.