Energy for Health, Vol. 22, 2022
Ryabko Ye.V., Bakhtereva Ye.V., Zuev S.L.
Yekaterinburg Medical Research Center for Prophylaxis and Health Protection in Industrial Workers, Yekaterinburg, Russian Federation
Introduction
Plantar fasciitis is a painful condition of the foot. It is defined as an inflammation of the plantar fascia, the fibrous envelope of the tendon that forms the arch of the foot (from the Latin “fascia”). The role of the plantar fascia is to support and protect the tendon on the sole of the foot.
Plantar fasciitis is one of the most common causes involving pain at the base of the heel. In the course of life, it affects up to 10% of the population. It usually lasts for at least 6 months, rarely reaching a year. The clinical course for most patients is positive, about 80% report a resolution of symptoms within 12 months. [Martin RL et al.]
Plantar fasciitis mostly affects the population between 40 and 60 years of age, the women and obese subjects. Plantar fasciitis mostly affects the women, obese subjects, athletes – especially runners and population between 40 and 60 years of age.
Among musculoskeletal injuries related to running, the incidence of plantar fasciitis varies between 4.5% and 10%, with a prevalence between 5.2% and 17.5%. [Lopes AD et al.]. Sudden increase in mileage out of proportion to training, incorrect running posture, wrong choice of running shoes, running on too hard ground, are all possible causes of plantar fasciitis development.
The precise mechanism of onset of plantar fasciitis is still being studied, as the research conducted so far reports conflicting data. Experts agree in considering this condition as the result of excessive stress on the plantar fascia which, if subjected to repeated stress and microtrauma over time, degenerates and becomes painful.
The diagnosis of plantar fasciitis can be made through the only physical examination; however, medical doctors (in alternative physicians) may also order imaging studies to clear up any doubts and to rule out other possible causes of heel pain.
Plantar fasciitis takes several months (6 to 12) for complete recovery from pain symptoms that, interfering with daily routine, could impair life quality. Among the therapies planned to solve this condition, there are: the pharmacological approach, aimed at affecting the symptoms of plantar fasciitis by administering non-steroidal anti-inflammatory drugs and corticosteroids; the “strengthening” approach with stretching and strengthening exercises and the use of specialized devices (splints, orthotics); the surgical approach and therapies based on the use of physical agents like extracorporeal shockwaves therapy (ESWT) and laser therapy.
Shock waves are pulsed acoustic waves that dissipate mechanical energy at the interface of two substances with different acoustic impedance. Such therapy has demonstrated good results in the treatment of patient affected by plantar fasciitis [Li et al.] but it is not free of collateral effects.
Roerdink et al. in their systematic-review on the complication of ESWT in plantar fasciitis, found that the 11.6% of the patients reported pain during the treatment. Dysesthesia, swelling, ecchymosis and/or petechiae, severe headache, bruising, throbbing sensation and temporary pain after treatment, <1 week from the treatment session end, were also been noticed. Laser therapy has been demonstrated to provide many beneficial effects through photochemical, photothermal and photomechanical interaction with the tissue.
Low-level laser therapy (LLLT) by class 3B lasers with Power <500 mW, in a recent systematic review [Guimarães et al.] demonstrated to be effective in the treatment of plantar fasciitis, reducing pain of 2.2 on a 0–10 pain scale and providing an average improvement in pain of 40%. Moreover, compared to extracorporeal shock wave therapy, LLLT resulted equivalent in reducing pain intensity in the short term.
In the last years High-intensity laser therapy (HILT) by class 4 laser source with power > 500 mW, has gained importance in the treatment of musculoskeletal disorders and sports injuries [Brown et al., Dundar et al.]. HILT has been recognized to be a safe, non-invasive and non-painful therapy.
Clinical evidence on the effects of HILT in combination with other phys ical therapies are limited despite treating patients with several therapies during the same treatment session and/or in succession, is becoming part of common practice.
Akkurt et al. evaluated the effects of HILT in combination with insole versus insole alone, in patients affected by chronic plantar fasciitis and found that the combined therapy was more effective than the sole insole in terms of pain and quality of life.
The purpose of this study was to evaluate the performance of ESWT, HILT and their combination, in patients with chronic heel pain, caused by plantar fasciitis, in terms of pain relief.
We hypothesize that the use of ESWT and HILT combined together in succession, during the same session treatment, could act synergically and lead more benefits in terms of: less invasiveness and pain symptoms after the treatment and higher antalgic, anti-inflammatory, anti-oedema, reparative and regenerative effects on deep structure.
Materials and Methods
This prospective, randomized, single center trial was conducted at the Yekaterinburg Medical Research Center for Prophylaxis and Health Protection in Industrial Workers of Yekaterinburg, Russia.
Data were collected from a group of 40 consecutive patients aged between 40-50 years, affected by chronic plantar fasciitis, lasting over 3 months, without any remission of signs and symptoms, pain over 4 on visual analogue scale (VAS).
The diagnosis was made through physical examination; the enthesopathy was evaluated by ultrasonic indicators: thickness of the plantar fascia, homogeneity, swelling, calcification, neovascularization. Figure 1.
No other inclusion or exclusion criteria have been used. The population was randomly divided in four groups: Group 1 (n=10) received placebo; Group 2 (n=10) was treated with HILT; Group 3 (n=10) was treated with ESWT; Group 4 (n=10) received ESWT+HILT combined.
Change of pain intensity from baseline to the end of the treatment sessions, as reported by the patients on a Visual Analogue Scale (VAS), in the four groups of treatment, were calculated and compared statistically. The VAS scores were collected before each treatment session.
Patient randomized in Group 4 received initially the treatment with ESWT and immediately after a treatment with HILT. This choice was made because HILT could alleviate the painful temporary sensation some patients feel after a ESWT session. Figure 2.
At one month, after the onset of the treatment cycle, the patients underwent to an ultrasound exam to evaluate changes of the swelling and plantar fascia structure
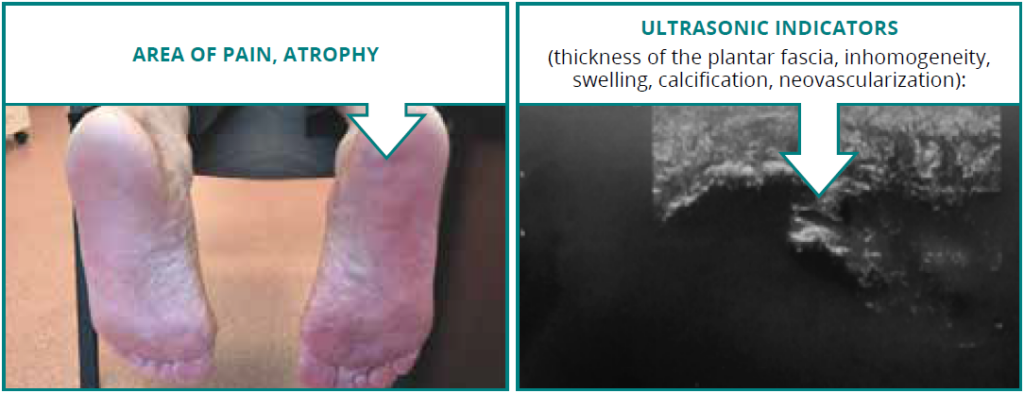
Figure 1
Area of pain and ultrasonic indicators characterized plantar fasciitis.

Figure 2
Group 4 – treatment with ESWT and HILT during the same session.
HILT Protocol
Pulsed high power laser (Nd:YAG, λ=1064nm, Hiro 3, ASA Laser, Arcugnano, Italy) was applied as 10 sessions performed daily in two weeks. All treatments were performed according to instructions in operating manual. Each session lasted 10-15 minutes and was divided in three phases: fast manual scanning, trigger point treatments and slow manual scanning. Each phase was done applying a fluency increasing / frequency decreasing emissions. The predefined plantar fasciitis settings were: fluency of 970-1080-1170 mJ/cm2, frequency of 30-20-10 Hz, total energy of 1000-1250-1500J.
ESWT Protocol
For ESWT therapy was used a Salus Optimus Pro (Madisson, s.r.o.), with radial shock waves, energy density of 2.5-3 bar, frequency set to 10-13Hz, and predefined plantar fasciitis treatment mode. All treatments were performed according to instructions in operating manual. Each patient received 5 treatments in 2 weeks: 3 treatments the first week and 2 the second one.
Results
At baseline, the patients in the four different groups were comparable by gender, age and severity of clinical manifestations.
Average pain intensity in the population under examination at baseline was 7.1±1.9 on a 0-10 scale.
At the end of the treatment cycle the patients who received HILT (Group 2) or HILT+ESWT (Group 4) reported a significant improvement of pain (p≤0.05). Patients treated with ESWT alone (Group 3) reported a decrease of pain on VAS scale but not significant; while, placebo group showed no improvement. All the results are showed in Figure 3 and Table 1.
In group 4, VAS scores before and after treatment were 7.1±1.2 and 2.1±1.1 respectively; already after a short period of time, 4.3±1.2 days, was achieved the greater drop in pain intensity. Ultrasounds performed at follow-up, one month after the onset of the treatment cycle, showed a reduced swelling and signs of structure repair in plantar fascia. Figure 4.
Patient of group 2, HILT monotherapy, significantly decreased pain in 8-10 days since the onset of the therapy; the VAS score before and at the end of the treatment cycle were 7.2±2.1 and 3.2±1.8 respectively. At follow-up the ultrasound exam presented a reduced swelling in plantar fascia. Figure 4.
In the group 3, the effects of ESWT emerged in over a 14 days’ period, in correspondence of the last treatment. The VAS score before treatment was 6.9±2.1, after treatment was 4.3±2.6. At follow-up visit no ultrasound changes were seen. No adverse events or side effects were recorded during the entire curse of the study.
Visual Analogue Scale (CM) Mean (STD)
| Baseline | End of Treatment | ΔVAS | p-value | |
|---|---|---|---|---|
|
Group 1 – Placebo |
7.3 |
7.2 |
0.1 |
NS |
|
Group 2 – HILT |
7.2 (2.1) |
3.2 (1.8) |
4 |
p<0.005 |
|
Group 3 – ESWT |
6.9 (2.1) |
4.3 (2.6) |
2.6 |
NS |
|
GROUP 4 – HILT+ESWT |
7.1 (1.2) |
2.1 (1.1) |
5 |
p<0.005 |
Table 1
VAS score values before and after the treatment.

Evaluation of the Visual Analogue Scale in the different groups before and after the treatment cycle sessions.

Figure 4
Ultrasound evaluation of the effects of HILT therapy alone or in combination with ESWT at follow-up.
Discussion
In this prospective study, patient with chronic plantar fasciitis, were treated with ESWT, HILT or with a combination of the two therapies and their effects on pain were evaluated.
The results showed a significant reduction of pain in patients treated with high-intensity laser therapy alone or in combination with the external shockwave therapy. In the group of patients treated with two therapies in combination, it was obtained the greatest reduction in pain in the shortest period of time.
These results are in line with those found by Takla et al. where 120 patients with chronic plantar fasciitis received either ESWT with photobiomodulation therapy (PBMT), ESWT (once a week), PBMT (three times a week), or sham-PBMT (three times a week) for three consecutive weeks. PBMT was provided with low level GaAlAs laser.
Both ESWT and PBMT showed an increase in pressure pain threshold values, a decrease of pain and an increase of functional ability. As we found, the application of PBMT in combination with ESWT resulted to be superior over ESWT and PBMT alone.
This could be related to a smaller number of treatment sessions and a relative shorter period before the evaluation of the therapy effects, 2 weeks instead of 3 weeks.
Our results sustain the hypothesis that HILT and ESWT in combination could lead to therapeutic mechanisms that potentiate each other, and that act synergistically.The shockwaves initiate a number of non-specific responses at tissue level both in correspondence of the front wave and at damping part of the wave. The front wave initiates the cleavage of chemical bonds within the components of cell membranes and alters the mechanical properties of cell membranes. These changes occur only in the damaged cells and cause their cytolysis (osmotic lysis).
The damping part of the shockwave stimulates metabolism, regeneration and immune processes within the damaged tissues. Resulting from the removal of dead cells and cellular debris by the macrophages and the edema resolution, the compression of nerve fibers and nerve receptors decreases. This ultimately relieves the pain.
The high intensity laser therapy uses a source with a low tissue absorption coefficient (Nd: YAG) with the
emission of impulses. The patented pulses, generated by the Hiro 3 device, are characterized by very high peak powers (1-3 kW), high energy content (150-130 mJ), short duration (120-150 μs), low frequency and duty cycle in the order of 0.1%.
The characteristics that differentiate the HILT from traditional therapies are: the wavelength – 1064nm, high peak power and short pulse duration. This can favorite the photomechanical and biological effects on the tissue [Monici et al.]
In this study HILT therapy demonstrated to be effective both alone and in combination with ESWT.
In particular, in this second scenario, it seems that the HILT administrated immediately after ESWT, could potentiate the positive effects emerging at the damping area, producing a greater and quicker improvement in pain respect to a monotherapy without any side effects.
Conclusions
HILT and ESWT are usually applied in physical therapy department alone or in combination; when applied together, showed significantly better results in managing chronic heel pain in patients with chronic plantar fasciitis, with regard to both reducing pain and structural repair of plantar fascia.
Bibliography
- Martin RL, Irrgang JJ, Conti SF. Outcome study of subjects with insertional plantar fasciitis. Foot Ankle Int. 1998;19:803-811.
- Lopes AD, Hespanhol Junior LC, Yeung SS, Costa LO. What are the main running-related musculoskeletal injuries? A systematic review. Sports Med. 2012;42:891-905. http://dx.doi.org/10.1007/BF03262301.
- Li, H., Xiong, Y., Zhou, W. et al. Shock-wave therapy improved outcome with plantar fasciitis: a meta-analysis of randomized controlled trials. Arch Orthop Trauma Surg 139, 1763–1770 (2019). https://doi.org/10.1007/s00402-019-03262-z.
- Roerdink, R L et al. “Complications of extracorporeal shockwave therapy in plantar fasciitis: Systematic review.” International journal of surgery (London, England) vol. 46 (2017): 133-145. doi:10.1016/j.ijsu.2017.08.587.
- Brown AW, Weber DC Physical agent modalities (2000) In: Braddom RL (ed) Physical medicine and rehabilitation. WB Saunders, Harcourt Health Sciences Company, London; pp 440-458.
- Dundar U, Turkmen U, Toktas H, Ulasli AM, Solak O (2015) Effectiveness of high-intensity laser therapy and splinting in lateral epicondylitis; a prospective, randomized, controlled study. Lasers Med 30: 1097-1107.
- Akkurt, F., Akkurt, H. E., Yilmaz, H., Olgun, Y., & Sen, Z. (2018). Efficacy of high-intensity laser therapy and silicone insole in plantar fasciitis. Int J Phys Med Rehabil, 6(484), 2.
- Guimarães, Janice S et al. “Effect of low-level laser therapy on pain and disability in patients with plantar fasciitis: A systematic review and meta-analysis.” Musculoskeletal science & practice vol. 57 (2022): 102478. doi:10.1016/j.msksp.2021.102478.
- Takla, Mary Kamal Nassif, and Soheir Shethata Rezk-Allah Rezk. “Clinical effectiveness of multi-wavelength photobiomodulation therapy as an adjunct to extracorporeal shockwave therapy in the management of plantar fasciitis: a randomized controlled trial.” Lasers in medical science vol. 34,3 (2019): 583-593. doi:10.1007/s10103-018-2632-4.
- Monici M., Cialdai F., Fusi F., Romano G., Pratesi R. “Effects of pulsed Nd:YAG laser at molecular and cellular level. A study on the basis of Hilterapia”. Energy for health vol. 3 (2009): 26-33.