Energy for Health, Vol. 25, 2025
Giacomo Insero1,2,* and Giovanni Romano1
1 Department of Experimental and Clinical Biomedical Sciences “Mario Serio", University of Florence, FI, Italy
2 CNR-INO - Istituto Nazionale di Ottica, Sesto Fiorentino FI, Italy
In the last few decades, we have witnessed a wide dissucion of intense optical sources such as lasers or LEDs (Light Emitting Diodes) [1]. These devices are now present not only in hospitals and research environments, but are now routinely deployed in non-hospital settings, including private outpatient clinics, such as dermatology and dental offices, aesthetic medical clinics, physiotherapy clinics, as well as veterinary practices. Depending on the specific therapeutic procedures, these light sources operate over wavelengths spanning from the UV (ultraviolet) to the mid-IR (mid-infrared) region.
Such diffusion exposes patients and operators to risks from artificial optical radiation, that must be properly assessed in the occupational safety framework [2]. Risk management must be robust not only in controlled operating theatres but also in smaller and decentralized clinical rooms, as less frequent use of these technologies may result in operators having limited experience with laser-based procedures, thereby inincreasing the likelihood of accidents or unsafe practices. In the veterinary context, laser sources may be used directly in the field, further complicating the implementation of standard risk-minimization measures. Training pathways commonly address these issues under workplace safety programs and are aligned with normative references and guidance documents: Directive 2006/25/EC (artificial optical radiation), ICNIRP exposure-limit guidelines (180 nm– 1,000 μm) [3], and device standards for medical laser equipment (e.g., EN 60601-2-22). These frameworks provide essential foundations for hazard identification, classification, and selection of controls and personal protective equipment (PPE).
However, in day-to-day clinical practice, training and checklists often emphasize prevention of direct-beam exposure and unexpected events, such as misalignment, accidental light-induced firing or device malfunction. A less underlined risk is connected to the reflected radiation generated during normal treatment, which can represent an important ocular hazard even when procedures are performed correctly. In this work, we underline the risks related to reflected laser radiation during routine treatments rather than exceptional or accidental events.
The Light Reflection
A common assumption in laser safety is that “if the primary beam is controlled (and everyone wears appropriate eyewear), residual risks are negligible”, but this is not necessarily true.
When an optical beam impinges on the interface between two media with refractive indices n1 and n2 — for instance, air and a solid, liquid, or a tissue (Figure 1) — a fraction of the incident radiant power is always reflected due to the refractive-index mismatch [4]. The remaining fraction enters the second medium (e.g. the tissue), where it may be attenuated by absorption and (in most cases) also by scattering. If the medium is not optically opaque at the wavelength of interest and the geometry allows it, a portion of the radiation can traverse the material and exit into air on the opposite side as transmitted radiation.
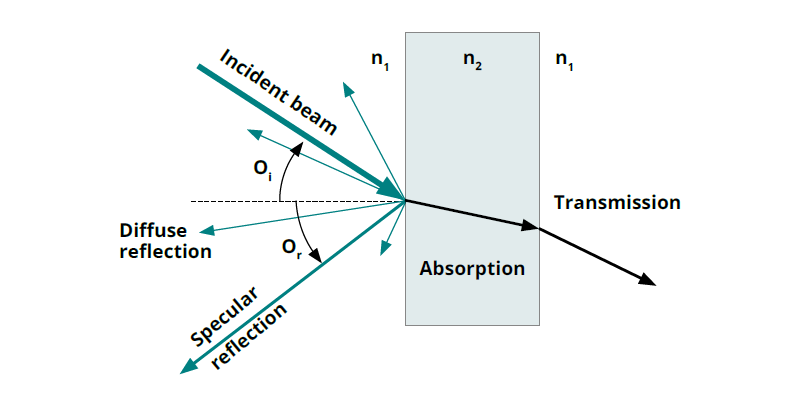
Figure 1
Scheme depicting the presence of both diffuse and specular reflected radiation.
When an optical beam impinges on the interface between two media with refractive indices n1 and n2 — for instance, air and a solid, liquid, or a tissue (Figure 1) — a fraction of the incident radiant power is always reflected due to the refractive-index mismatch [4]. The remaining fraction enters the second medium (e.g. the tissue), where it may be attenuated by absorption and (in most cases) also by scattering. If the medium is not optically opaque at the wavelength of interest and the geometry allows it, a portion of the radiation can traverse the material and exit into air on the opposite side as transmitted radiation.
For a given wavelength λ, these processes can be described by the spectral reflectance R(λ), transmittance T(λ), and absorptance A(λ), which satisfy the energy balance
R(λ) + T(λ) + A(λ) = 1,
where each quantity is defined as the ratio of reflected, transmitted, or absorbed radiant power to the incident radiant power, respectively. Therefore, they are dimensionless, ranging from 0 (for example R = 0 means no reflected radiation) to 1 (for example R = 1 means all the incident power is reflected).
Depending on the surface characteristics, reflection may be sub-divided into:
- Specular reflection: directional, mirror-like; the reflected angle equals the incidence angle. This component corresponds to a secondary beam able to propagate over long distances and potentially maintaining the majority of incident beam energy, according to the value of R.
- Diffuse reflection: scattered into many directions. In strongly scattering surfaces, typically approximated as Lambertian, the specular reflection is strongly reduced, and the total reflected energy is distributed over a large solid angle.
Following this division, the total reflectance R(λ) = Rtot (λ)lambda) can also be split as
RTot (λ) = RS (λ) + RD (λ)
where RS (λ) and RD (λ) represent the specular and diffusive reflectance components, respectively. As RS (λ) depends on the incidence angle of the light, we have decided to focus our discussion on RS 45° (λ), corresponding to the specular reflectance at the exemplary incidence angle of 45°. This angle is representative of many practical situations and is also easily measurable with simple and inexpensive setups. Following our work on [5], we can identify a simple parameter that immediately indicates whether a surface mainly exhibits specular or diffusive characteristics, and we call it the Lambertian parameter LLamb (λ) defined as
LLamb (λ) = 100 · [ (RS 45° (λ) / RS 45° (λ) + RD (λ) ]
For most of the materials, LLamb ranges between 1 and 100: low values indicate predominantly diffusing materials, while higher values indicate specular behavior. Since LLamb depends on the wavelength, the same material can have a predominantly diffusive or rather specular behavior according to the wavelength or wavelength range considered. In fact, the reflective characteristic of a material depends on its microstructure and the ratio between the characteristic surface roughness and λ. Surfaces that are smooth on the scale of λ tend toward specular reflection; increasing roughness promotes scattering and diffuse behavior. Importantly, a surface may appear “non-shiny” in visible light yet behave more specularly at longer wavelengths where the same roughness becomes small relative to λ. Especially in the NIR range, one cannot reliably infer infrared reflectance behavior from visible appearance. A frequent oversimplification in laser safety is to equate “diffuse” with “safe” due to the reduced irradiance in any single direction compared with a specular reflection, but diffuse reflection can still pose risks when incident powers are high, and distances surface-to-eye are short. Risks associated to specular reflection could be underestimated because they extend ocular hazard beyond what would be intuitively expected for “indirect exposure.”
In realistic geometries in clinical settings, the beam frequently encounters several different surfaces: the patient’s tissue, surgical drapes, plastic accessories, metallic instruments, endoscope components, dental mirrors, or smooth polymer housings. These interactions, which include multi-bounce paths, can create non-negligible reflected, and often uncontrolled, components that may enter an operator’s visual field. In the following, we show reflectance and Lambertian parameters of materials commonly found in biomedical/clinical environments, measured over a broad spectral range (250 nm to 25 μm), explicitly separating specular and diffuse components [5].
Clinically Relevant Materials: Metals, Textiles, Plastic and Polymers
- Metals (e.g., stainless steel clinical instruments):
Metallic instruments are ubiquitous in procedural fields. They can be both “polished” or satin finished. Polished surface are mirror-like and they have high-specular reflectance as high as almost 100 %, as expected; nevertheless, also brushed or satin metals can exhibit specular reflection in the visible range up to few tens of percentage, which is not negligible considering high-power sources.
In the mid-infrared (2.4–25 μm), reflectance measurements showed that brushed metals can exhibit higher reflectance in the 10–25 μm range compared to the visible range up to several tens of percentage points. This is particularly relevant to CO₂ lasers (~10.6 μm) and other NIR systems, as also shown by the Lambert parameter plot [5].
Operational implication: where possible, minimize exposed metallic surfaces in the illuminated field; prefer matte/blackened tools or use non-reflective covers when compatible with sterility and procedure constraints.
- Surgical Textiles and Field Drapes
Blue/green surgical clothing and coverings are often assumed to be “safe” if irradiated because they don’t show a perceivable specular reflectance (generally less than 4% in the 250–2500 nm range). Nevertheless, these textiles can have high total reflectance: in the 0.7- 2.5 um range, many tested fabrics showed total reflectance typically ~60% to nearly 90% depending on fabric type and composition. The average Lambertian parameter over 400–1100 nm is generally lower than 10, confirming the strongly diffusive reflective nature of these materials.
Operational implication: diffuse does not mean irrelevant. Closerange scattering from high-power systems can still pose ocular concerns if eyewear is absent or not properly chosen or if scattered beam reaches the eye through lateral gaps.
- Plastics and Polymers (Device Housings, Disposable, etc.)
Polymers such as plexiglass (PMMA), polycarbonate, PVC, and PTFE are common in clinical settings (protective shields, device enclosures, tubing, disposable accessories, positioning tools) and exhibit generally diffuse reflective behavior, but if polished can have a high specular reflection. The average Lambertian parameter in the range 250 nm -2.5 μm can be higher than 80 for polished PVC, plexiglass or polycarbonate, indicating a high specular reflectance component against a total reflectance of approx. 10-20%. Indeed, PTFE components show diffusive behavior, LLamb (λ) ~ 2. While generally less hazardous than polished metals, these materials can still reflect a substantial fraction of incident radiation.
Operational implication: smooth polymer and transparent plastic surfaces can present a reflection that, while possibly modest in absolute terms, is highly specular in character— hence potentially hazardous.
Beam Properties Matter: Collimated Versus Focused Emission
A further practical point is that reflection hazards cannot be assessed based solely on surface type; they must be coupled to the spatial properties of the employed laser beam:
- Collimated beams (low divergence): a specular reflection tends to remain collimated, preserving radiant exposure over long distances. In this case, a secondary specular reflection can behave as a “mirror-generated beam” that remains hazardous even far from the reflection point.
- Focused beams: the hazard depends strongly on where the focus is relative to reflective surfaces and human eye. A specular reflection from a surface near the focal region may still carry high irradiance, while reflections far from focus may be less intense due to divergence—yet can remain non-negligible for high-power settings.
Operational implication: the risk from specular reflection is not governed only by “how shiny” a surface is; it depends on the laser’s divergence, spot size, and working distance as well. Therefore, device-specific information (beam diameter, divergence, focusing optics, delivery system) should be explicitly included in the clinical risk assessment.
These considerations reinforce the importance of appropriate personal protective equipment. Laser safety eyewear should provide adequate attenuation at the operating wavelength and ensure full coverage, including lateral protection. In addition, unnecessary metallic or plastic objects should be removed from the illuminated field whenever possible.
Concluding Remarks
Reflected radiation should be treated as a first-order element of clinical laser safety, not as a residual concern limited to mishaps. Reflected laser radiation represents a tangible ocular hazard in clinical environments, even during routine and correct use of medical laser devices. While diffuse reflections are generally less dangerous than specular ones, their contribution cannot be neglected, particularly at nearinfrared wavelengths.
Acknowledgements
We thank Luca Mercatelli, Cristina Cimmino, Andrea Guasti, Nidia Maldonado Carmona, and Franco Fusi for data collection and analysis, and Roberto Gaetano Donato for administrative supportBibliography
- Keiser G. Fundamentals of Light Sources. In: Biophotonics. Graduate Texts in Physics. Springer, Singapore; 2022.
- Barat K. Understanding Laser Accidents, CRC Press Taylor Francis Group, United States, 2019.
- International Commission on Non-Ionizing Radiation Protection (ICNIRP). ICNIRP Guidelines on Limits of Exposure to Laser Radiation of Wavelengths between 180 nm and 1,000 μm. Health Physics. 2013;105(3):271–295. doi:10.1097/HP.0b013e-3182983fd4
- M. H. Niemz, Laser-Tissue Interactions, Springer, Berlin New York, 4th ed., 2019
- Insero G, Fusi F, Romano G. The safe use of lasers in biomedicine: Principles of laser-matter interaction. Journal of Public Health Research. 2023;12(3). doi: 10.1177/22799036231187077